19 March 2021: Clinical Research
Association Between Body Mass Index and Thyroid Function in Euthyroid Chinese Adults
Jing Fu1ACE, Lin Zhang1BDF, Yu An1C, Yan Duan1B, Jia Liu1ADE*, Guang Wang12AFDOI: 10.12659/MSM.930865
Med Sci Monit 2021; 27:e930865






Abstract
BACKGROUND: Obesity can influence thyroid function through multiple routes, even in people who are euthyroid. The correlation between weight and thyroid function is a matter of debate. The present study investigated the relationship between body weight and thyroid function in euthyroid Chinese adults.
MATERIAL AND METHODS: A total of 1564 participants with serum thyrotropin (TSH) and thyroid hormone levels within the reference range were included. All of them were tested for thyroid function parameters and categorized, based on body mass index (BMI), into 3 groups: normal weight, overweight, and obese. The effects of BMI on thyroid function were examined using linear (continuous values) and logistic (dichotomous levels according to medians or means) regression and controlling for age and sex.
RESULTS: There were significant differences in free triiodothyronine (FT3) levels and FT3/free thyroxine (FT4) ratios among participants who were normal weight, overweight, and obese (both P<0.001). Multivariable regression analysis (P<0.001) showed that BMI was positively associated with FT3 levels and FT3/FT4 ratios. Compared with the normal weight group, the patients who were overweight or obese had significantly higher FT3 levels and FT3/FT4 ratios that were higher than average, according to logistic regression analyses.
CONCLUSIONS: We found that Chinese adults who are obese may have higher FT3 levels and FT3/FT4 ratios than those who are of normal weight, even if their thyroid function values are within the normal range.
Keywords: Body Mass Index, Obesity, Thyroid Function Tests, Asians, Body Weight, overweight, Thyroid Gland, Thyroid Hormones, thyrotropin, thyroxine, Triiodothyronine
Background
Obesity is becoming a worldwide epidemic disease and it is highly prevalent in developed countries. An estimated 30% of the adult population in the United States is obese; in the UK, the proportion is 25% [1–3]. In developing countries, with growth in their economies, the incidence of obesity has been shown to rise rapidly. Between 2002 and 2012, the prevalence of obesity in Chinese adults increased from 7.1% to 11.9% and the overall prevalence of obesity and overweight increased from 29.9% to 42% [4].
Previous studies have revealed that the effects of obesity on the endocrine system are multifaceted, although that is seldom noted. Obesity can affect thyroid function and the release of gonadotropin releasing hormone (GnRH), alter the luteinizing hormone pulse amplitude [5], decrease growth hormone levels, and increase cortisol levels. Thyroid function is closely related to obesity and obesity-related metabolic disease. Therefore, increasing attention is being focused on the effects of obesity on thyroid function.
Several studies have explored alterations in thyroid function associated with differences in body mass index (BMI) in individuals who are euthyroid [6–10]. The results, however, have been rather inconsistent. Most of these studies have had small sample sizes and concentrated on the effects of thyroid function on BMI. We aimed to investigate the effects of BMI on thyroid function in the present cross-sectional study with a relatively large sample size in China.
Material and Methods
SUBJECTS AND METHODS:
For the present study, 1564 adults aged 18 to 70 years were recruited between November 2018 and November 2019 at Beijing Chaoyang Hospital, Capital Medical University. All of them were asked about their medical histories and they received physical examinations and underwent laboratory tests. The exclusion criteria included known history of cardiovascular disease or diabetes; thyroid dysfunction, use of hormone replacement therapy such as thyroid or sex hormones; use of antithyroid treatment; antithyroid peroxidase antibody (TPOab) titers ≥60; severe hepatic or renal insufficiency; use of weight loss medications, antihypertensive or lipid-lowering drugs, glucocorticoids or amiodarone; and moderate-to-severe anemia, cancer, acute infection, and pregnancy.
Anthropometric measurements (weight and height) were taken of all participants. Free triiodothyronine (FT3), free thyroxine (FT4), and thyroid-stimulating hormone (TSH) levels were measured with a chemiluminescence immunoassay (ADVIA Centaur XP, Siemens Healthcare Diagnostics, Germany). Anti-thyroglobulin antibody (TgAb) and TPOab were detected with a chemiluminescence immunoassay (ADVIA Centaur XP, Siemens Healthcare Diagnostics, Germany). High-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), triglycerides (TG), and fasting blood glucose were measured with colorimetric enzymatic assays using an autoanalyzer (ADVIA 2400, Siemens Healthcare Diagnostics, Germany). Total cholesterol (TC) levels were detected with an enzymatic method, TG levels with a glycerol lipase oxidase reaction, and HDL-C and LDL-C were assayed directly. Fasting serum insulin (FINS) was measured with a chemiluminescence immunoassay using a Centaur XP immunoassay system (Siemens Healthcare Diagnostics, Germany). White blood cells (WBCs), lymphocytes, neutrophils, and platelet counts were measured using an automatic hemocyte analyzer (Sysmex XE-5000, Japan). BMI was calculated using the formula: BMI=weight/(height squared)(kg/m2). The formula for the Homeostatic Model Assessment for Insulin Resistance (HOMA-IR) was as follows: [FBG (mmol/L)×FINS (mIU/L)/22.5]; Homeostasis model assessment of β-cell function (HOMA-β)=20×FINS (mIU/L)/[FBG (mmol/L)–3.5]. The neutrophil-to-lymphocyte ratio (NLR) was calculated as NLR=neutrophil count/lymphocyte count. The participants were divided into 3 groups: normal weight (BMI 18.5–23.9 kg/m2), overweight (BMI 24.0–27.9 kg/m2), and obese (BMI ≥28 kg/m2).
The protocol for the present study was approved by the Ethics Committee of Beijing Chaoyang Hospital. All of the participants signed the informed consent form. The protocol was implemented in accordance with provisions of the Declaration of Helsinki.
STATISTICAL ANALYSIS:
All data were analyzed using Stata software, version 13.1. Variables that followed a normal distribution are shown as means±standard deviations. Differences among groups were evaluated with an analysis of variance test. In post hoc analyses, a Tukey test was used for pairwise comparisons. Variables that did not follow a normal distribution – including FINS, TgAb, TPOab, and TG – are presented as medians (first quartile to third quartile). Data that were not normally distributed were evaluated using non-parametric statistics. Correlation analyses were performed using Pearson’s correlation test and the non-parametric Spearman rank correlation test as appropriate. Associations between BMI and thyroid function as continuous variables were assessed using linear regression models. Associations between different BMI groups and indices of thyroid function, which were divided into dichotomous variables according to medians or means, were investigated using logistic regression models. The results are given as odds ratios (95% confidence intervals [CIs]) or standardized β coefficients.
Results
A total of 1564 participants were included in the final analysis, of whom 468 were women. Demographics and baseline characteristics of the participants are shown in Table 1. BMI was 22.77±1.65, 27.01±1.34 and 32.07±1.98 kg/m2 (
Table 1 shows that thyroid function differed among the 3 groups. FT3 levels were 5.28±0.54, 5.36±0.56 and 5.46±0.52 pmol/L in the groups who were of normal weight, overweight, and obese, respectively (
Table 2 shows the relationships between thyroid parameters and laboratory indices. We found that TSH, FT3, and FT3/FT4 were significantly correlated with FINS, HOMA-IR, and HOMA-β, respectively. FT3/FT4 was negatively correlated with TC, HDL-C, and NLR. FT4 was positively associated with WBC and neutrophil counts. After adjustment for age and sex, multivariable regression analysis showed no significant correlations between BMI and FT4 or between BMI and TSH, but BMI was positively correlated with FT3 and FT3/FT4 (both
After adjustment for age and sex, logistic regression analyses showed that, compared with normal weight, both overweight and obesity were significantly associated with an increased risk of higher FT3 (ORs 1.350 and 1.875, respectively) as were FT3/FT4 ratio (ORs 1.415 and 2.118, respectively). Also compared with normal weight, obesity was associated with an increased risk of a higher TSH level (OR 1.609, 95% CI 1.113–2.285) (Table 3).
Discussion
Prior studies have noted the importance of the relationship between obesity and thyroid dysfunction. However, reports on the exact relationship between obesity and thyroid function are limited and inconsistent. Fontenelle et al summarized multiple studies published between 2005 and 2015 on the status of thyroid hormones in euthyroid obese adults [11]. Half of the studies (9/19) reported a significant positive correlation between BMI and TSH, whereas the other half did not. Similarly, half of the studies (6/11) found a positive correlation between BMI and FT3 or total triiodothyronine. Of the 16 studies, only 3 reported a negative correlation between BMI and FT4.
The present study was designed to assess the association between BMI and thyroid function in euthyroid Chinese adults. Our results showed positive associations between BMI and FT3 levels and between BMI and FT3/FT4 ratios. However, no statistically significant differences in FT4 levels were found among the different BMI groups.
The mechanism and clinical implications of the changes in thyroid function associated with obesity have not yet been fully elucidated. At present, obesity is believed to affect thyroid function via several mechanisms, including dysfunction of adipose tissue, effects of hyperinsulinemia, and changes in thyroid gland structure and function. Several studies have suggested that dysfunction of adipose tissue is the major factor responsible for variations in the homeostasis of thyroid hormones [12–15].
Adipose tissue, which is endocrine in nature, can produce and secrete leptin. Patients who are obese have higher leptin levels than those who are not obese. Leptin plays an important role in thermoregulation and energy balance and interacts with thyroid hormones. A defect in leptin secretion could affect the rhythm of TSH secretion. In addition, leptin could promote the expression of thyrotropin-releasing hormone messenger RNA. Leptin could trigger an increase in the number of thyroid cells by binding to the leptin receptor on the cells [16]. In addition, leptin also can modulate deiodinase activity in different organs, thereby affecting the level of thyroid hormone [17–22]. These mechanisms, in part, may underly the elevated FT3/FT4 ratios and FT3 levels in the group in the present study that was obese.
On the other hand, thyroid hormones within the euthyroid range are also found to be involved in metabolic diseases. Xu et al conducted a study with 16 975 subjects and found that thyroid function could influence body weight and contribute to the development of obesity [23]. Thyroid hormone influences body weight through regulation of resting energy expenditure but the precise mechanism has not been fully clarified [24]. Although not all resting energy expenditure is thyroid hormone-dependent, minor changes in thyroid hormone levels have a significant effect on resting energy expenditure. For instance, resting energy expenditure decreases by 75 to 150 kcal/d, while serum TSH concentration increases by 0.5 to 1 mIU/L, which is still within the normal range. If this change persists over the long term, it can result in significant weight gain [25].
Clearly, the interactions between thyroid function and insulin sensitivity are complex and multifaceted. Our data suggest that FINS levels, HOMA-IR, and HOMA-β are associated with thyroid function. Our results are consistent with other research, which shows that thyroid function can be influenced by insulin resistance in obese, euthyroid individuals. The putative mechanism is the potential contribution of obesity-associated insulin resistance to reduction in deiodinase enzyme D2 activity in thyrotrophic cells, which leads to changes in the levels of thyroid hormones [26–28].
Obesity is recognized as a chronic, low-grade, inflammatory condition. Several inflammatory markers, such as WBC, neutrophil, and lymphocyte counts, are found to increase in people who are obese [29,30]. Although the mechanism by which WBCs and neutrophils affect thyroid function is not well known, a recent study found that these inflammatory markers play some role in the development of nodular thyroid disease [31].
The number of participants in the present study was small, particularly in the group that was obese. A possible reason is that individuals who are obese often pay less attention to their health and are less inclined to have check-ups than their counterparts who are not obese. Therefore, with a relatively small sample size, we did not find a linear association between BMI and TSH levels. Nevertheless, using logistic regression analyses, we still found that obese individuals were more likely to have higher TSH levels than those who were normal weight, indicating that BMI may have an effect on TSH levels only in patients who are obese.
Conclusions
In conclusion, we observed that Chinese adults who were obese had higher FT3 levels and FT3/FT4 ratios compared with those who were of normal weight, even though their thyroid function was within the normal range. These findings will help us to better understand changes in thyroid function that accompany an increase in body fat. Because the present study was cross-sectional, no direct causal associations can be inferred. Therefore, longitudinal studies are needed to thoroughly elucidate the complex interplay between body weight and thyroid function that is within the normal range.
Figures
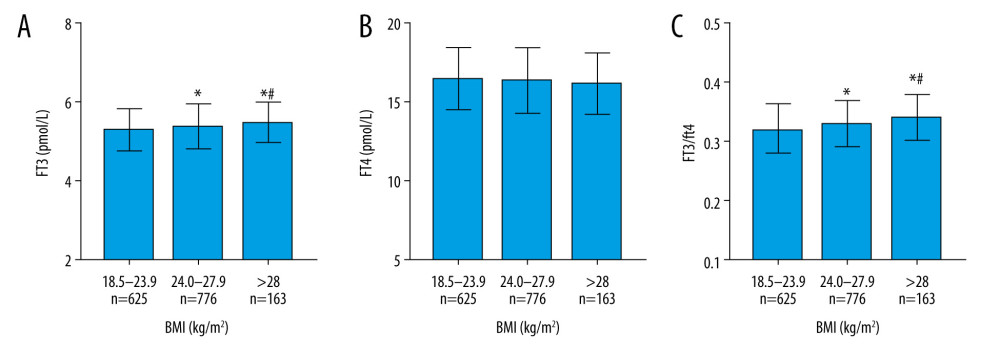 Figure 1. Association between body mass index and thyroid function in euthyroid Chinese adults. (A) Association between body mass index (BMI) and free triiodothyronine (FT3) level in euthyroid Chinese adults. (B) Association between BMI and free thyroxine (FT4) level. (C) Association between BMI and FT3/FT4 ratio. Compared with the normal weight group, * significantly different at P<0.05 and ** significantly different at P<0.01. Compared with the overweight group, # significantly different at P<0.05 and ## significantly different at P<0.01.
Figure 1. Association between body mass index and thyroid function in euthyroid Chinese adults. (A) Association between body mass index (BMI) and free triiodothyronine (FT3) level in euthyroid Chinese adults. (B) Association between BMI and free thyroxine (FT4) level. (C) Association between BMI and FT3/FT4 ratio. Compared with the normal weight group, * significantly different at P<0.05 and ** significantly different at P<0.01. Compared with the overweight group, # significantly different at P<0.05 and ## significantly different at P<0.01. 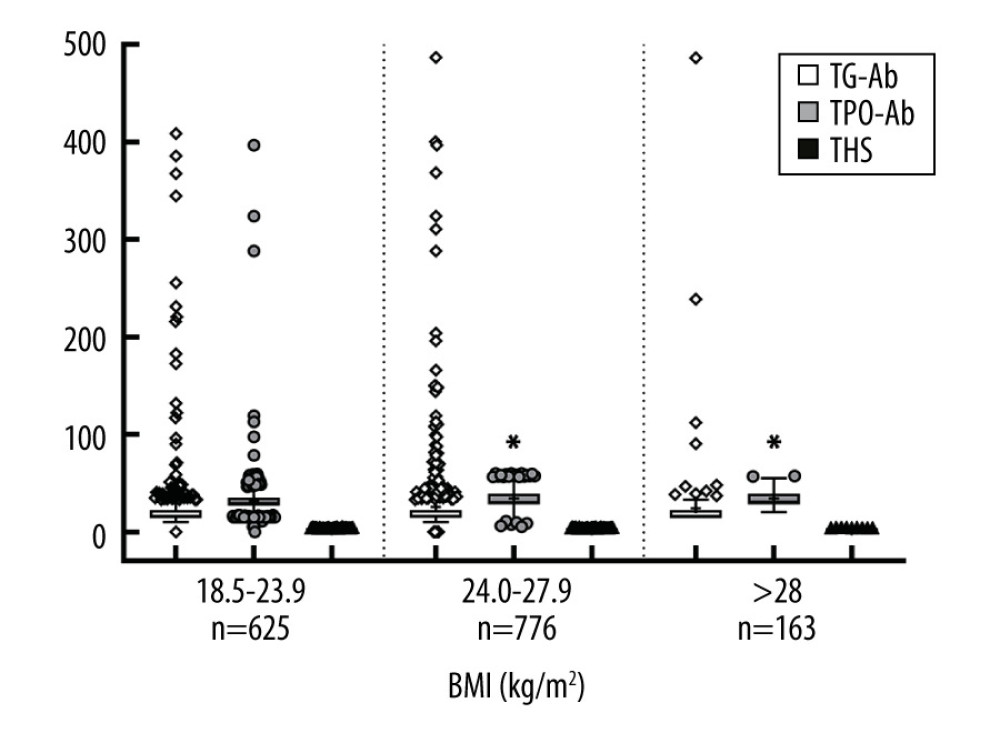 Figure 2. Serum thyrotropin, antithyroid peroxidase antibody, and antithyroglobulin antibody levels in groups with different body mass indexes. Compared with the normal weight group, * significantly different at P<0.05.
Figure 2. Serum thyrotropin, antithyroid peroxidase antibody, and antithyroglobulin antibody levels in groups with different body mass indexes. Compared with the normal weight group, * significantly different at P<0.05. References
1. Ryan DH, Kahan S, Guideline recommendations for obesity management: Med Clin North Am, 2018; 102; 49-63
2. Tsai AG, Williamson DF, Glick HA, Direct medical cost of overweight and obesity in the USA: A quantitative systematic review: Obes Rev, 2011; 12; 50-61
3. Ng M, Fleming T, Robinson M, Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: A systematic analysis for the Global Burden of Disease Study 2013: Lancet, 2014; 384; 766-81
4. The Chinese National Health and Family Planning Commission: The Nutrition and Health Status of the Chinese People (2015 Report)
5. Michalakis K, Mintziori G, Kaprara A, The complex interaction between obesity, metabolic syndrome and reproductive axis: A narrative review: Metabolism, 2013; 62; 457-78
6. Bétry C, Challan-Belval MA, Bernard A, Increased TSH in obesity: Evidence for a BMI-independent association with leptin: Diabetes Metab, 2015; 41; 248-51
7. Kitahara CM, Platz EA, Ladenson PW, Body fatness and markers of thyroid function among U.S.men and women: PLoS One, 2012; 7; e34979
8. Lambrinoudaki I, Armeni E, Rizos D, Indices of adiposity and thyroid hormones in euthyroid postmenopausal women: Eur J Endocrinol, 2015; 173; 237-45
9. Santini F, Marzullo P, Rotondi M, Mechanisms in endocrinology: the crosstalk between thyroid gland and adipose tissue: Signal integration in health and disease: Eur J Endocrinol, 2014; 171; R137-52
10. Pearce EN, Thyroid hormone and obesity: Curr Opin Endocrinol Diabetes Obes, 2012; 19; 408-13
11. Fontenelle LC, Feitosa MM, Severo JS, Thyroid function in human obesity: underlying mechanisms: Horm Metab Res, 2016; 48; 787-94
12. Muscogiuri G, Sorice GP, Mezza T, High-normal TSH values in obesity: Is it insulin resistance or adipose tissue’s guilt: Obesity (Silver Spring), 2013; 21; 101-6
13. Ren R, Jiang X, Zhang X, Association between thyroid hormones and body fat in euthyroid subjects: Clin Endocrinol (Oxf), 2014; 80; 585-90
14. Lips MA, Pijl H, van Klinken JB, Roux-en-Y gastric bypass and calorie restriction induce comparable time-dependent effects on thyroid hormone function tests in obese female subjects: Eur J Endocrinol, 2013; 169; 339-47
15. Nannipieri M, Cecchetti F, Anselmino M, Expression of thyrotropin and thyroid hormone receptors in adipose tissue of patients with morbid obesity and/or type 2 diabetes: Effects of weight loss: Int J Obes (Lond), 2009; 33; 1001-6
16. Isozaki O, Tsushima T, Nozoe Y, Leptin regulation of the thyroids: Negative regulation on thyroid hormone levels in euthyroid subjects and inhibitory effects on iodide uptake and Na+/I− symporter mRNA expression in rat FRTL-5 cells: Endocr J, 2004; 51(4); 415-23
17. Cabanelas A, Lisboa PC, Moura EG, Acute effects of leptin on 5′-deiodinases are modulated by thyroid state of fed rats: Horm Metab Res, 2007; 39; 818-22
18. Cabanelas A, Lisboa PC, Moura EG, Leptin acute modulation of the 5′-deiodinase activities in hypothalamus, pituitary and brown adipose tissue of fed rats: Horm Metab Res, 2006; 38; 481-85
19. Araujo RL, Carvalho DP, Bioenergetic impact of tissue-specific regulation of iodothyronine deiodinases during nutritional imbalance: J Bioenerg Biomembr, 2011; 43; 59-65
20. Araujo RL, Andrade BM, Padrón AS, High-fat diet increases thyrotropin and oxygen consumption without altering circulating 3,5,3′-triiodothyronine (T3) and thyroxine in rats: The role of iodothyronine deiodinases, reverse T3 production, and whole-body fat oxidation: Endocrinology, 2010; 151; 3460-69
21. Ortega FJ, Jílková ZM, Moreno-Navarrete JM, Type I iodothyronine 5′-deiodinase mRNA and activity is increased in adipose tissue of obese subjects: Int J Obes (Lond), 2012; 36; 320-24
22. Macek Jílková Z, Pavelka S, Flachs P, Modulation of type I iodothyronine 5′-deiodinase activity in white adipose tissue by nutrition: possible involvement of leptin: Physiol Res, 2010; 59; 561-69
23. Xu R, Huang F, Zhang S, Thyroid function, body mass index, and metabolic risk markers in euthyroid adults: a cohort study: BMC Endocr Disord, 2019; 19; 58
24. Silva JE, Thyroid hormone control of thermogenesis and energy balance: Thyroid, 1995; 5; 481-92
25. al-Adsani H, Hoffer LJ, Silva JE, Resting energy expenditure is sensitive to small dose changes in patients on chronic thyroid hormone replacement: J Clin Endocrinol Metab, 1997; 82; 1118-25
26. Schauer PR, Kashyap SR, Wolski K, Bariatric surgery versus intensive medical therapy in obese patients with diabetes: N Engl J Med, 2012; 366; 1567-76
27. Kullmann S, Heni M, Hallschmid M, Brain insulin resistance at the crossroads of metabolic and cognitive disorders in humans: Physiol Rev, 2016; 96; 1169-209
28. Galofré JC, Pujante P, Abreu C, Relationship between thyroid-stimulating hormone and insulin in euthyroid obese men: Ann Nutr Metab, 2008; 53; 188-94
29. Ren Z, Zhao A, Wang Y, Association between dietary inflammatory index, c-reactive protein and metabolic syndrome: A cross-sectional study: Nutrients, 2018; 10(7); 831
30. Meng G, Zhu Q, Shao J, Comparing the diagnostic ability of inflammatory markers in metabolic syndrome: Clin Chim Acta, 2017; 475; 1-6
31. Li Z, Zhang L, Huang Y, Yang P, A mechanism exploration of metabolic syndrome causing nodular thyroid disease: Int J Endocrinol, 2019; 2019; 9376768
Figures
Figure 1. Association between body mass index and thyroid function in euthyroid Chinese adults. (A) Association between body mass index (BMI) and free triiodothyronine (FT3) level in euthyroid Chinese adults. (B) Association between BMI and free thyroxine (FT4) level. (C) Association between BMI and FT3/FT4 ratio. Compared with the normal weight group, * significantly different at P<0.05 and ** significantly different at P<0.01. Compared with the overweight group, # significantly different at P<0.05 and ## significantly different at P<0.01.Figure 2. Serum thyrotropin, antithyroid peroxidase antibody, and antithyroglobulin antibody levels in groups with different body mass indexes. Compared with the normal weight group, * significantly different at P<0.05. Tables
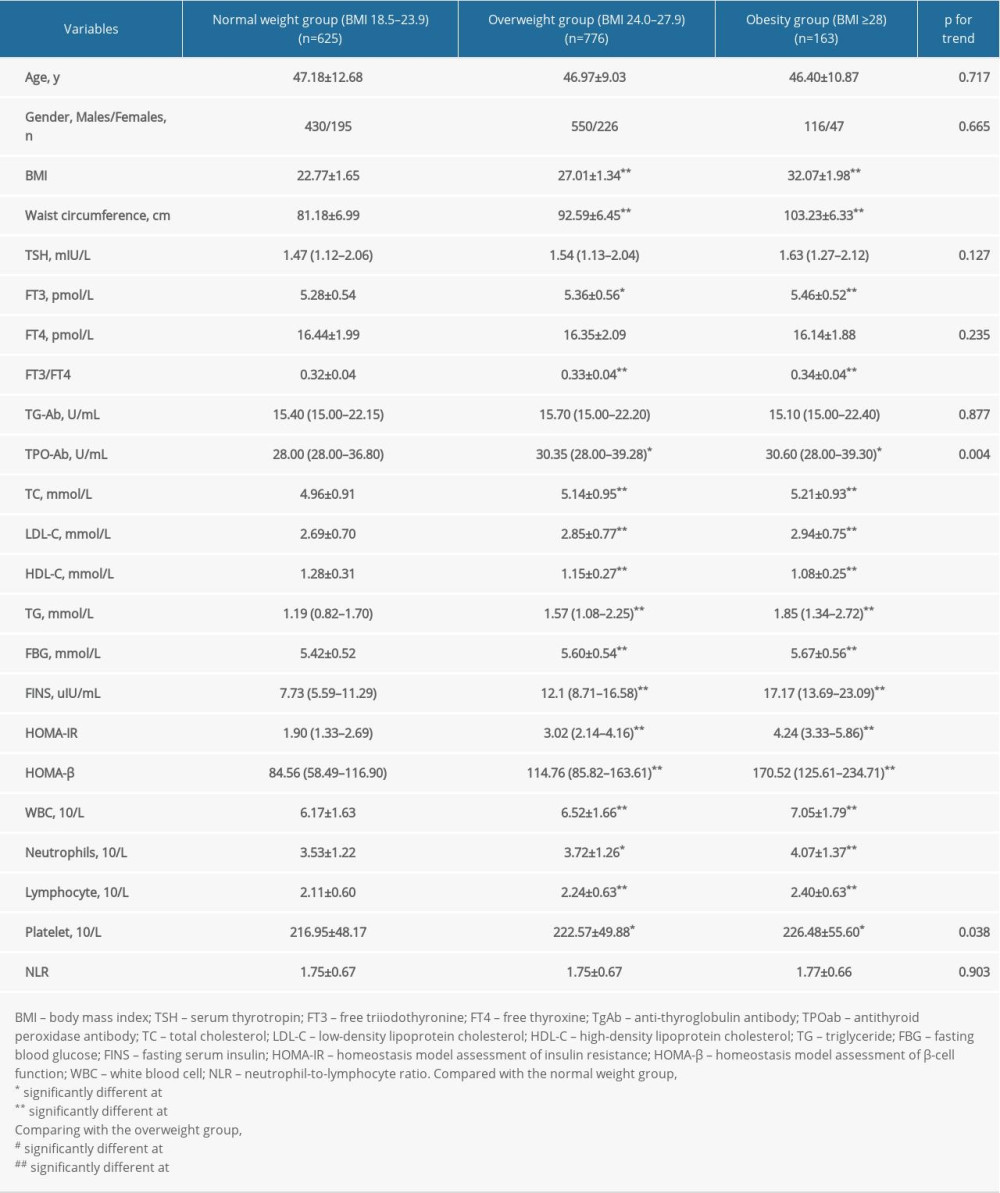 Table 1. Characteristics of euthyroid Chinese adults with various levels of body weight.
Table 1. Characteristics of euthyroid Chinese adults with various levels of body weight.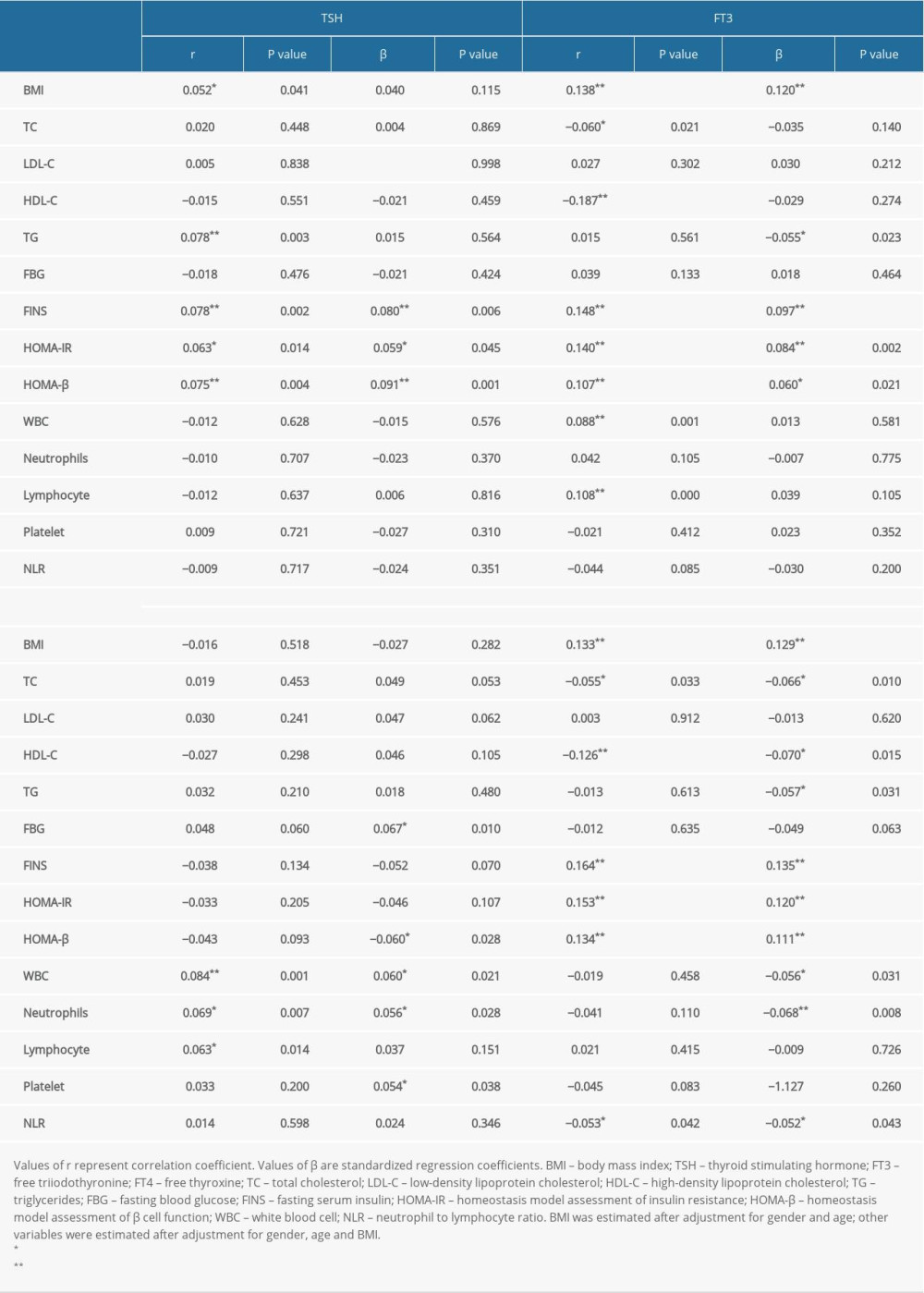 Table 2. Associations between thyroid function and laboratory indices.
Table 2. Associations between thyroid function and laboratory indices.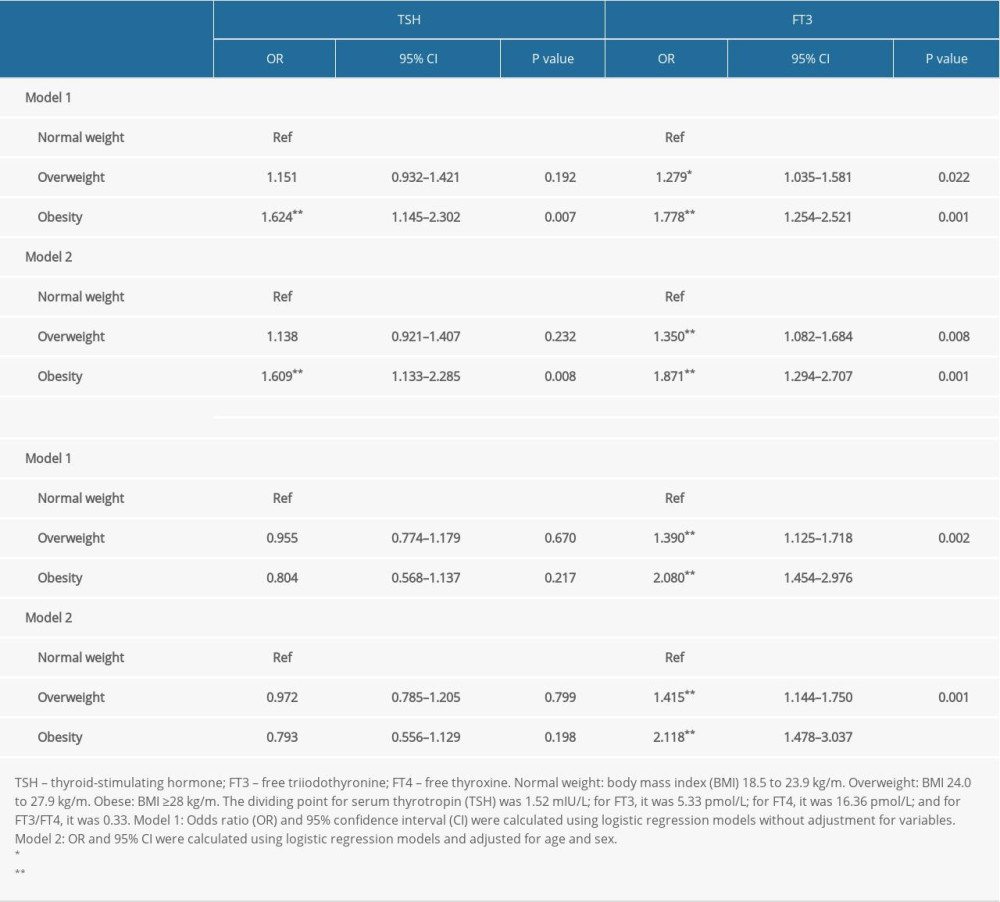 Table 3. Logistic regression analyses of the risk of higher levels of indices for thyroid function.Table 1. Characteristics of euthyroid Chinese adults with various levels of body weight.Table 2. Associations between thyroid function and laboratory indices.Table 3. Logistic regression analyses of the risk of higher levels of indices for thyroid function.
Table 3. Logistic regression analyses of the risk of higher levels of indices for thyroid function.Table 1. Characteristics of euthyroid Chinese adults with various levels of body weight.Table 2. Associations between thyroid function and laboratory indices.Table 3. Logistic regression analyses of the risk of higher levels of indices for thyroid function. In Press
Clinical Research
Modified Thoracoabdominal Nerves Block Through the Perichondrial Approach vs Subcostal Transversus Abdomini...Med Sci Monit In Press; DOI: 10.12659/MSM.953976
Clinical Research
Establishment of a Novel Approach for Drug Abuse Monitoring and Its Application in Medical InstitutionsMed Sci Monit In Press; DOI: 10.12659/MSM.952054
Database Analysis
Epidemiology of Incidence and Mortality Due to Head and Neck Cancer in Poland in 2000 to 2022Med Sci Monit In Press; DOI: 10.12659/MSM.952477
Clinical Research
Comparison of Outcomes From Sequential Endoscopic Therapy in 60 Patients With Cirrhosis and Esophagogastric...Med Sci Monit In Press; DOI: 10.12659/MSM.952290
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,658
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,764,203
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,395
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,966
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387