07 August 2021: Clinical Research
A Retrospective Study of 268 Patients with SARS-CoV-2 Infection to Evaluate the Association Between Blood Glucose and Severity of COVID-19 Pneumonia and Patient Mortality
Yaoyao Sun12CDE, Nan Jiang1ABD, Zhijun LiDOI: 10.12659/MSM.932156
Med Sci Monit 2021; 27:e932156






Abstract
BACKGROUND: Diabetes is one of the most commonly reported comorbidities among patients infected with SARS-CoV-2. This retrospective study of patients with SARS-CoV-2 infection was conducted to evaluate the association between blood glucose levels and the severity of COVID-19 pneumonia and patient mortality.
MATERIAL AND METHODS: A total of 268 patients with confirmed SARS-CoV-2 infection were included in this retrospective study. We obtained demographic characteristics, clinical symptoms, laboratory data, and survival information from patients’ electronic medical records. Blood glucose was measured on admission to the hospital. Comorbidities, including hypertension, diabetes, chronic kidney disease, chronic liver disease, chronic obstructive pulmonary disease, and cardiovascular disease, were collected by self-reported medical history.
RESULTS: Significantly higher risks of severe COVID-19 were found in patients with blood glucose levels ranging from 5.53 to 7.27 mmol/L (odds ratio [OR], 3.98; 95% confidence interval [CI], 1.81-8.75) and in patients with blood glucose ≥7.27 mmol/L (OR, 12.10; 95% CI, 5.53-26.48) than in those with blood glucose <5.53 mmol/L. There was a trend toward better survival in patients with blood glucose <5.53 mmol/L than in patients with blood glucose from 5.53 to 7.27 mmol/L (hazard ratio [HR], 6.34; 95% CI, 1.45-27.71) and ≥7.27 mmol/L (HR, 19.37; 95% CI, 4.68-80.17). Estimated 10-day overall survival rates were 96.8%, 90.6%, and 69.3% in patients with blood glucose <5.53 mmol/L, 5.53 to 7.27 mmol/L, and ³7.27 mmol/L, respectively.
CONCLUSIONS: Hyperglycemia was association with severity of COVID-19 pneumonia and with increased patient mortality. These findings support the need for blood glucose monitoring and control of hyperglycemia in patients with COVID-19 pneumonia.
Keywords: Blood Glucose, COVID-19, Hyperglycemia, severe acute respiratory syndrome coronavirus 2, Blood Glucose Self-Monitoring, COVID-19, Comorbidity, Hospital Mortality, Hospitalization, Proportional Hazards Models, Risk Factors, SARS-CoV-2, Severity of Illness Index, Survival Rate
Background
In December 2019, COVID-19 occurred in Wuhan, Hubei Province, China. Severe acute respiratory syndrome corona virus 2 (SARS-CoV-2) has been regarded as the pathogen causing COVID-19 disease, which mainly invades the respiratory tract and lungs [1]. Severe COVID-19 disease can rapidly trigger acute, even lethal, lung failure [2].
Diabetes is a major cause of mortality worldwide. The association between infection and diabetes has long been demonstrated, and patients with diabetes have a poorer progression and prognosis once infected than those without diabetes [3]. Diabetes and uncontrolled blood glucose levels can affect mortality in cases of SARS-CoV infection [4]. In addition, patients with diabetes are more likely to be infected with other bacteria and viruses, including
Therefore, this retrospective study of patients with SARS-CoV-2 infection was conducted to evaluate the association between blood glucose levels and the severity of COVID-19 pneumonia and patient mortality.
Material and Methods
STUDY POPULATION:
A total of 268 patients with confirmed COVID-19 were treated at Tongji Hospital from February 2 to March 25, 2020, in this retrospective study. All patients met the inclusion criteria: (1) epidemiology history, (2) positive result for SARS-Cov-2 RNA by real-time polymerase chain reaction (PCR) or positive results of SARS-CoV-2 IgM and IgG antibodies in serum specimens, and (3) chest computed tomography (CT) finding abnormalities indicative of viral pneumonia. Patients were excluded when there was missing data on blood glucose levels or on the severity of COVID-19 disease. SARS-CoV-2 was examined by real-time reverse transcription PCR (RT-PCR) assay. The real-time RT-PCR assay was performed using a 2019-nCoV nucleic acid detection kit, according to the manufacturer’s protocol (Sichuan Maccura Biotech Co., Ltd., China). Recorded information included demographic data, clinical symptoms, laboratory data, and survival information from patients’ electronic medical records. The Ethics Committee of Tongji Hospital (Wuhan, China) and China-Japan Union Hospital of Jilin University approved this study.
DEFINITIONS:
The hexokinase method was used to measure fasting blood glucose levels, which were measured after overnight fasting and before breakfast. The standard reference range was 3.9 to 6.1 mmol/L. Comorbidities, including hypertension, diabetes, chronic kidney disease, chronic liver disease, chronic obstructive pulmonary disease, and cardiovascular disease, were based on the patients’ self-reported medical history. Patients were divided into a severe COVID-19 group and a nonsevere COVID-19 group. Classification of severe COVID-19 required at least 1 of the following criteria: (1) respiratory rate ≥30/min, (2) finger oxygen saturation ≤93% in a resting state, (3) arterial oxygen tension/inspiratory oxygen fraction ≤300 mmHg, and (4) clinical symptoms that were gradually aggravated, with lung imaging showed that the lesions progressed >50% within 24 to 48 h [11]. Survival time was the time between admission and discharge from the hospital or death. The primary outcome was defined as the in-hospital mortality of patients with COVID-19.
STATISTICAL ANALYSIS:
The differences in baseline characteristics between the groups were measured using the Pearson chi-squared test or Fisher’s exact test for categorical variables and the
Results
BASELINE CHARACTERISTICS OF PATIENTS:
A total of 268 patients with COVID-19 were included in this retrospective study. Among these patients, 96 patients had severe COVID-19, and 172 patients had nonsevere COVID-19. The patients’ baseline characteristics are shown in Table 1. The median age of all patients was 58 years (range 20–88 years; interquartile range, 67–73 years), and 51.9% were men. Patients with severe COVID-19 were older than those with nonsevere COVID-19 (70 years vs 65 years) and had a higher percentage of men (60.4% vs 47.1%). We had comorbidity data for only 109 patients, with 61 of 109 patients having a history of comorbidities. In the severe COVID-19 group, 38 patients had comorbidities, and 23 patients had comorbidities in the nonsevere COVID-19 group; no significant differences were found in comorbidities between the 2 groups (P>0.05). Patients with severe COVID-19 also had higher neutrophil and leukocyte counts and higher blood glucose, aspartate transaminase (AST), alanine transaminase, lactate dehydrogenase (LDH), total bilirubin, and creatinine levels and lower lymphocyte counts than patients with nonsevere COVID-19 (P<0.05). We did not observe a significant difference in duration of hospitalization between the 2 groups.
ASSOCIATION BETWEEN BLOOD GLUCOSE AND SEVERE COVID-19:
When blood glucose was assessed by tertiles, significantly higher risks of severe COVID-19 were found in patients with blood glucose levels ranging from 5.53 to 7.27 mmol/L (OR, 3.98; 95% CI, 1.81–8.75) and in patients with blood glucose levels ≥7.27 mmol/L (OR, 12.10; 95% CI, 5.53–26.48) than in patients with blood glucose levels <5.53 mmol/L. After adjusting for sex and age by logistic regression, the ORs were 3.43 (95% CI, 1.53–7.70) and 8.82 (95% CI, 3.92–19.83), respectively (Table 2).
SURVIVAL ANALYSIS OF PATIENTS WITH COVID-19:
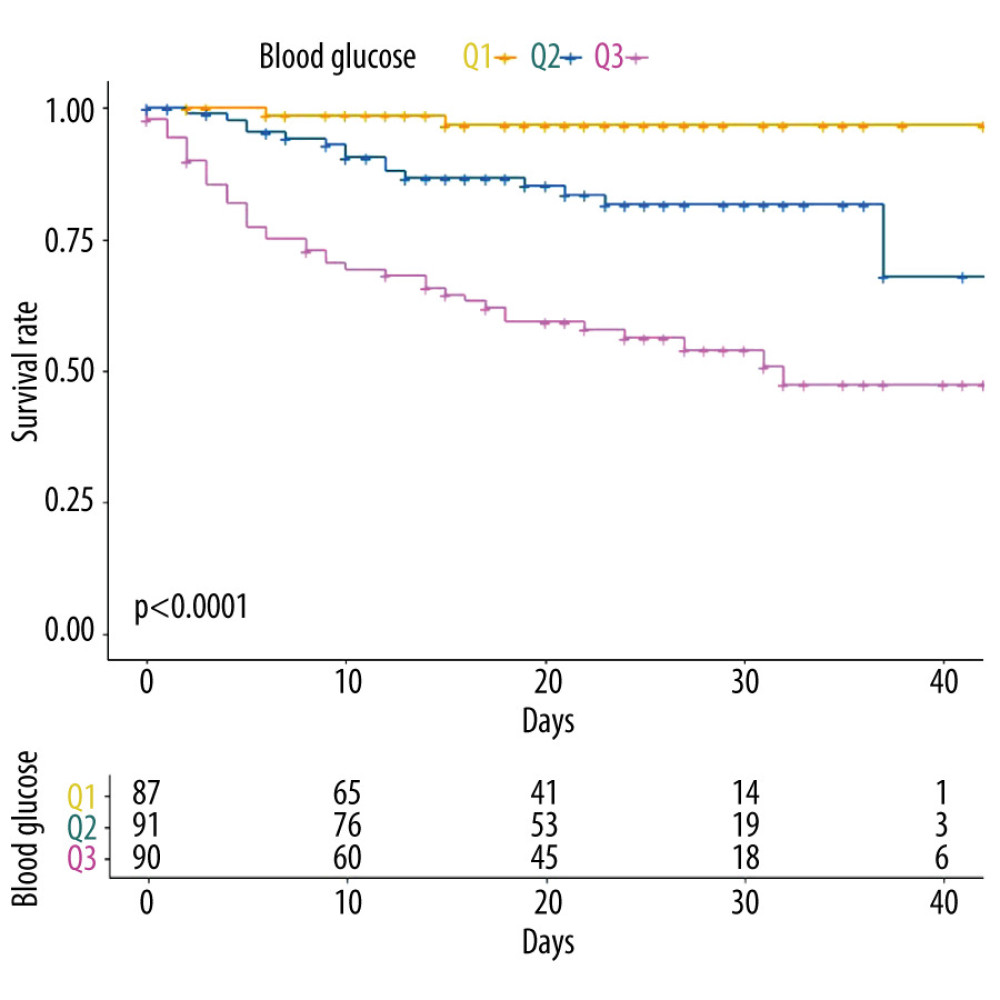
The survival curve of patients with COVID-19 is shown in Figure 1. This curve showed a trend toward better overall survival (OS) in patients with blood glucose levels of <5.53 mmol/L than in patients with blood glucose levels ranging from 5.53 to 7.27 mmol/L (hazard ratio [HR], 6.34; 95% CI, 1.45–27.71) and ≥7.27 mmol/L (HR, 19.37; 95% CI, 4.68–80.17). The estimated 10-day OS rates were 96.8%, 90.6%, and 69.3% in patients with blood glucose levels of <5.53 mmol/L, 5.53 to 7.27 mmol/L, and ≥7.27 mmol/L, respectively. Patients with blood glucose <5.53 mmol/L and patients with blood glucose levels ranging from 5.53 to 7.27 mmol/L did not reach the median survival time. The median survival duration was 32 days in patients with blood glucose levels of ≥7.27 mmol/L. The univariate log-rank test showed that several covariates were significantly associated with OS, including leukocyte, neutrophil, and lymphocyte counts and blood glucose, AST, LDH, total bilirubin, and creatinine levels (P<0.05). In multivariate Cox regression analysis, patients with blood glucose levels of ≥7.27 mmol/L had poorer OS than those with blood glucose levels of <5.53 mmol/L (HR, 10.13; 95% CI, 2.37–43.31). However, there was no difference in OS between patients with blood glucose levels of <5.53 mmol/L and patients with blood glucose levels ranging from 5.53 to 7.27 mmol/L (HR, 4.22; 95% CI, 0.94–19.01) (Table 3).
Discussion
Diabetes is one of the leading comorbidities association with the severity of 3 coronavirus infections, including MERS-CoV, SARS-CoV, and SARS-CoV-2. A previous study showed that compared with patients without diabetes, patients with diabetes have a 50% higher risk of death from COVID-19 [12]. In this retrospective study of SARS-CoV-2 infection, we found a positive association between blood glucose levels and the risk of severe COVID-19. A similar trend was found in survival analysis. Patients in the highest tertile of blood glucose levels had the lowest survival rates. In other words, the higher the blood glucose level, the greater the risk of severe disease or death.
The significant laboratory findings were elevated leukocyte and neutrophil counts and low lymphocyte counts in patients with severe COVID-19, compared with those with nonsevere COVID-19. One study observed that patients with COVID-19 have markedly low lymphocyte counts [13]. Poorly controlled diabetes is related to the inhibition of the lymphocyte proliferative response to different stimuli, release of interleukin 10, and the reduction in the fluidity, chemotaxis, and phagocytosis of polymorphonuclear leukocytes. With the increase of glycosylated hemoglobin A1c, the glycosylation degree of immunoglobulin in patients with diabetes increases, which directly damages the biological function of antibodies. When patients were grouped according to whether they had diabetes or not, several studies revealed that the lymphocyte counts of patients with diabetes are remarkably lower than those without diabetes, while leukocyte and neutrophil counts are higher [14,15]. In multivariate Cox regression analysis, we found neutrophils and lymphocytes were independent prognostic factors for mortality in patients with COVID-19.
A study conducted by Zhu et al showed that all-cause mortality in patients with COVID-19 with well-controlled blood glucose levels was significantly lower than that of those with poorly controlled blood glucose [16]; this is consistent with our study. Diabetes can be further aggravated after viral infection. Diabetes combined with SARS-CoV-2 infection can cause higher stress conditions and release more hyperglycemic hormones, leading to a dramatic fluctuation of blood glucose levels and abnormal blood glucose variability [17]. SARS-CoV and SARS-CoV-2 invade cells by binding to the angiotensin-converting enzyme 2 (ACE2) receptors of host cells [18]. The ACE2 protein is widely expressed in the human body, including in the heart and respiratory tract [19]. A study showed that immunostaining of ACE2 was stronger in islets than in exocrine tissues, suggesting that ACE2 protein is present in islet B cells and SARS-Cov-2 may cause hyperglycemia by damaging islets [20]. Therefore, COVID-19 cases with hyperglycemia have worse outcomes. The more severe cases of COVID-19 were in men in the present study. The expression of ACE2 protein in men was almost 3 times higher than that in women [14], which may be the reason men are more susceptible to severe COVID-19.
It is very important to monitor blood glucose levels and strengthen blood glucose control to reduce the severity of disease and mortality in patients with diabetes and SARS-CoV-2 infection. The results of our study showed that patients with blood glucose levels of <5.53 mmol/L had the lowest risk of severe disease and mortality. However, this does not mean that the lower the blood sugar, the better the outcome. Hypoglycemia can mobilize proinflammatory monocytes and increase the reactivity of platelets, leading to higher cardiovascular mortality in patients with diabetes.
Zhu et al found that maintaining glycemic variability between 3.9 mmol/L and 10.0 mmol/L is associated with reduced adverse outcomes and mortality [16].
There are several limitations in our study. First, the history of comorbidities of some patients with COVID-19 was not obtained owing to the difficulty of data collection; therefore, we did not include the history of comorbidities in the univariate and multivariate survival analysis. Second, this retrospective study has a small sample size, so the conclusions should be extended to other populations with caution.
Conclusions
The findings from this retrospective study showed that hyperglycemia was association with the severity of COVID-19 pneumonia and increased patient mortality. These findings support the need for blood glucose monitoring and control of hyperglycemia in patients with COVID-19 pneumonia.
References
1. Chen N, Zhou M, Dong X, Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study: Lancet, 2020; 395(10223); 507-13
2. Guan WJ, Ni ZY, Hu Y, Clinical characteristics of coronavirus disease 2019 in China: N Engl J Med, 2020; 382(18); 1708-20
3. Pearson-Stuttard J, Blundell S, Harris T, Diabetes and infection: Assessing the association with glycaemic control in population-based studies: Lancet Diabetes Endocrinol, 2016; 4(2); 148-58
4. Yang JK, Feng Y, Yuan MY, Plasma glucose levels and diabetes are independent predictors for mortality and morbidity in patients with SARS: Diabet Med, 2006; 23(6); 623-28
5. Smit J, Søgaard M, Schønheyder HC, Diabetes and risk of community-acquired Staphylococcus aureus bacteremia: A population-based case-control study: Eur J Endocrinol, 2016; 174(5); 631-39
6. Ahmed M, Omer I, Osman SM, Ahmed-Abakur EH, Association between pulmonary tuberculosis and type 2 diabetes in Sudanese patients: Int J Mycobacteriol, 2017; 6(1); 97-101
7. Banik GR, Alqahtani AS, Booy R, Rashid H, Risk factors for severity and mortality in patients with MERS-CoV: Analysis of publicly available data from Saudi Arabia: Virol Sin, 2016; 31(1); 81-84
8. Goyal P, Choi JJ, Pinheiro LC, Clinical characteristics of COVID-19 in New York City: N Engl J Med, 2020; 382(24); 2372-74
9. Wang D, Hu B, Hu C, Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus-infected pneumonia in Wuhan, China: JAMA, 2020; 323(11); 1061-69
10. Mirzaei F, Khodadadi I, Vafaei SA, Importance of hyperglycemia in COVID-19 intensive-care patients: Mechanism and treatment strategy: Prim Care Diabetes, 2021; 15(3); 409-16
11. National Health Commission of the People’s Republic of China: 8th edition of Diagnosis and Treatment Guideline of COVID-19, 2020 [in Chinese]http://www.nhc.gov.cn/cms-search/downFiles/a449a3e2e2c94d9a856d5faea2ff0f94.pdf
12. Remuzzi A, Remuzzi G, COVID-19 and Italy: What next?: Lancet, 2020; 395(10231); 1225-28
13. Huang C, Wang Y, Li X, Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China: Lancet, 2020; 395(10223); 497-506
14. Yan Y, Yang Y, Wang F, Clinical characteristics and outcomes of patients with severe COVID-19 with diabetes: BMJ Open Diabetes Res Care, 2020; 8(1); e001343
15. Guo W, Li M, Dong Y, Diabetes is a risk factor for the progression and prognosis of COVID-19: Diabetes Metab Res Rev, 2020 [Online ahead of print]
16. Zhu L, She ZG, Cheng X, Association of blood glucose control and outcomes in patients with COVID-19 and pre-existing type 2 diabetes: Cell Metab, 2020; 31(6); 1068-77.e3
17. Wang A, Zhao W, Xu Z, Gu J, Timely blood glucose management for the outbreak of 2019 novel coronavirus disease (COVID-19) is urgently needed: Diabetes Res Clin Pract, 2020; 162; 108118
18. Wan Y, Shang J, Graham R, Receptor recognition by the novel coronavirus from Wuhan: An analysis based on decade-long structural studies of SARS coronavirus: J Virol, 2020; 94(7); e00127-20
19. Song Z, Xu Y, Bao L, From SARS to MERS, thrusting coronaviruses into the spotlight: Viruses, 2019; 11(1); 59
20. Yang JK, Lin SS, Ji XJ, Guo LM, Binding of SARS coronavirus to its receptor damages islets and causes acute diabetes: Acta Diabetol, 2010; 47(3); 193-99
Tables
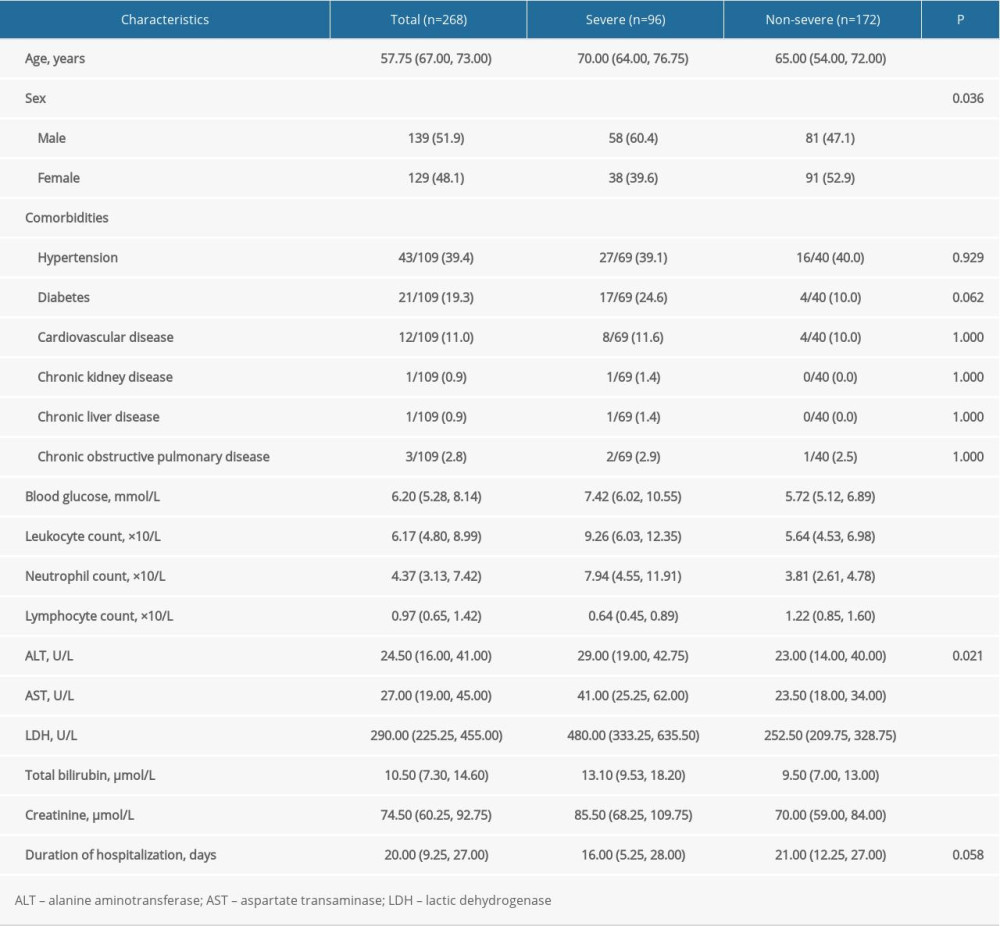 Table 1. The baseline characteristics of patients with COVID-19 (n, interquartile range, or percentage).
Table 1. The baseline characteristics of patients with COVID-19 (n, interquartile range, or percentage).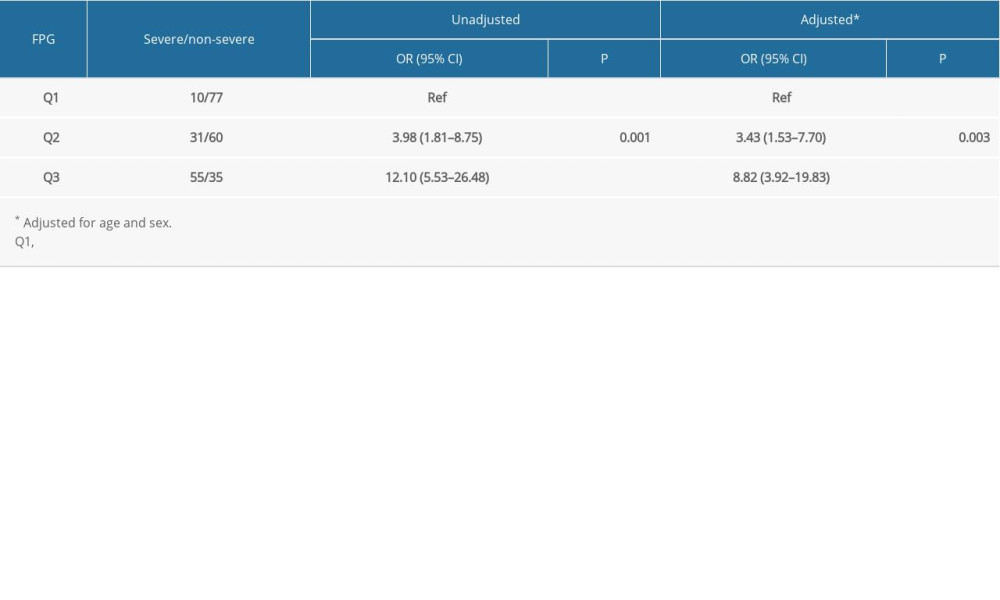 Table 2. Relationship of blood glucose with the risk of severe COVID-19.
Table 2. Relationship of blood glucose with the risk of severe COVID-19.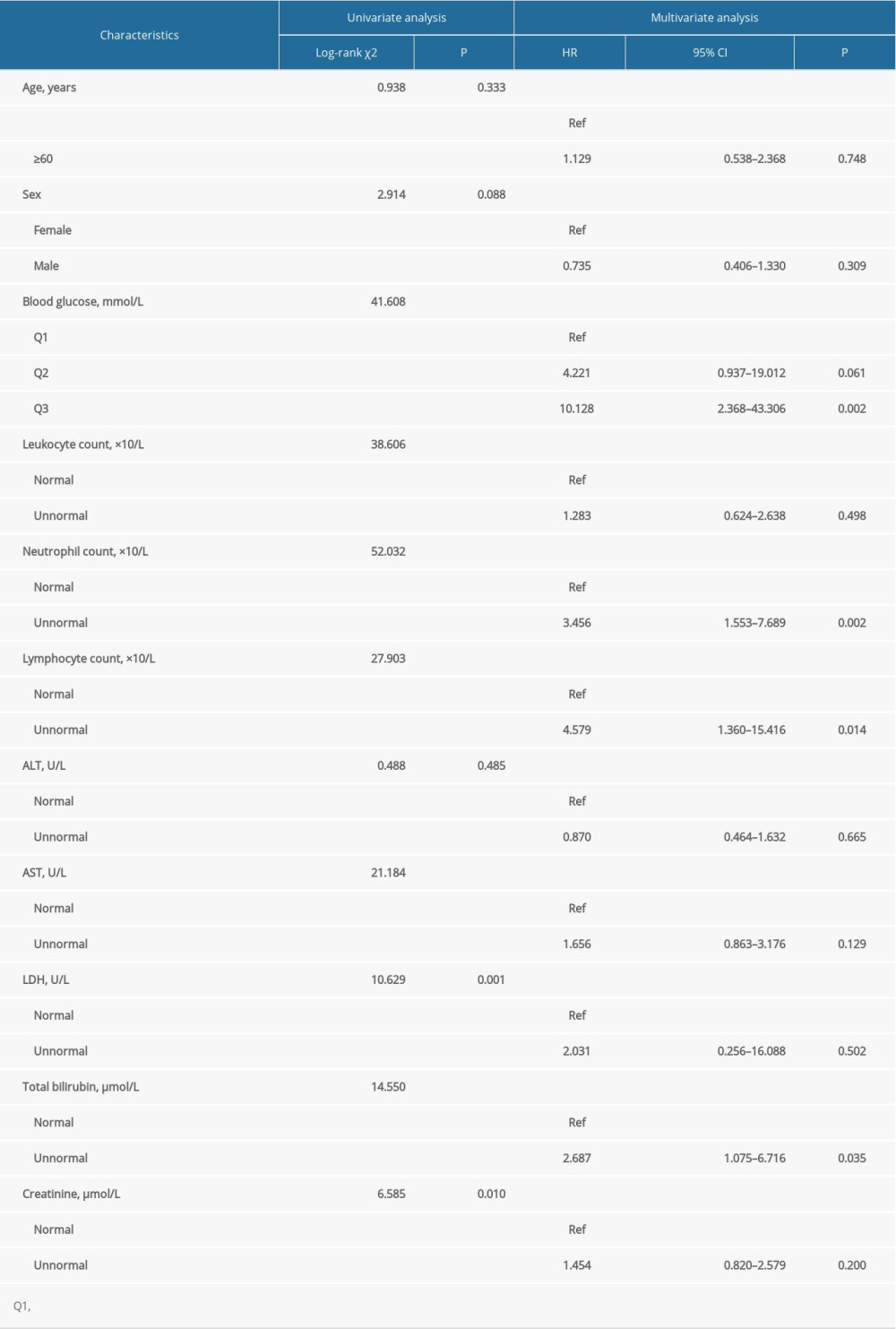 Table 3. Univariate and multivariate survival analysis of overall survival in patients with COVID-19.Table 1. The baseline characteristics of patients with COVID-19 (n, interquartile range, or percentage).Table 2. Relationship of blood glucose with the risk of severe COVID-19.Table 3. Univariate and multivariate survival analysis of overall survival in patients with COVID-19.
Table 3. Univariate and multivariate survival analysis of overall survival in patients with COVID-19.Table 1. The baseline characteristics of patients with COVID-19 (n, interquartile range, or percentage).Table 2. Relationship of blood glucose with the risk of severe COVID-19.Table 3. Univariate and multivariate survival analysis of overall survival in patients with COVID-19. In Press
Clinical Research
Institutional and Regional Variations in Access to Clinical Trials and Next-Generation Sequencing in Turkis...Med Sci Monit In Press; DOI: 10.12659/MSM.951027
Clinical Research
Low-Intensity Blood Flow-Restricted Multi-Joint Exercise Improves Muscle Function in Patients With Patellof...Med Sci Monit In Press; DOI: 10.12659/MSM.950516
Review article
Musculoskeletal Ultrasound and MRI in the Evaluation of Chemotherapy-Induced Peripheral Neuropathy: A ReviewMed Sci Monit In Press; DOI: 10.12659/MSM.951283
Clinical Research
Sensory Processing, Dissociation, and Affective Symptoms in Misophonia: A Cross-Sectional Study of 35 AdultsMed Sci Monit In Press; DOI: 10.12659/MSM.950938
Most Viewed Current Articles
17 Jan 2024 : Review article 10,187,196
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,708,487
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,341,643
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 706,524
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387