16 November 2020: Clinical Research
A Mobile App for Diabetes Management: Impact on Self-Efficacy Among Patients with Type 2 Diabetes at a Community Hospital
Yangkui Zhai1ABEG*, Wenjuan Yu2EFDOI: 10.12659/MSM.926719
Med Sci Monit 2020; 26:e926719






Abstract
BACKGROUND: Patients with type 2 diabetes upload and review blood glucose data between clinic visits. Many mobile phone applications (apps) that receive data from a “connected” glucometer and that support pattern management are available and have the capacity to make data upload and review less burdensome. The objective of this study was to assess whether the diabetic management app could improve glycemic control and diabetes self-efficacy in a Chinese community hospital by a randomized controlled trial.
MATERIAL AND METHODS: One-hundred twenty patients with type 2 diabetes registered at the Community Health Service Center of Zhangjiawo Town, Xiqing District, Tianjin City, China were recruited and volunteered to participate in the project. They were randomly divided into the mobile app intervention group (n=60) and the control group (n=60) for a 6-month observation. The control group was given conventional diabetic treatment and the app group was given the mobile app and conventional care. Self-efficacy was measured by the Diabetes Self-Efficacy Scale questionnaire. The differences between the 2 groups in hemoglobin A1c (HbA1c) and diabetes self-efficacy were evaluated at the third and sixth months.
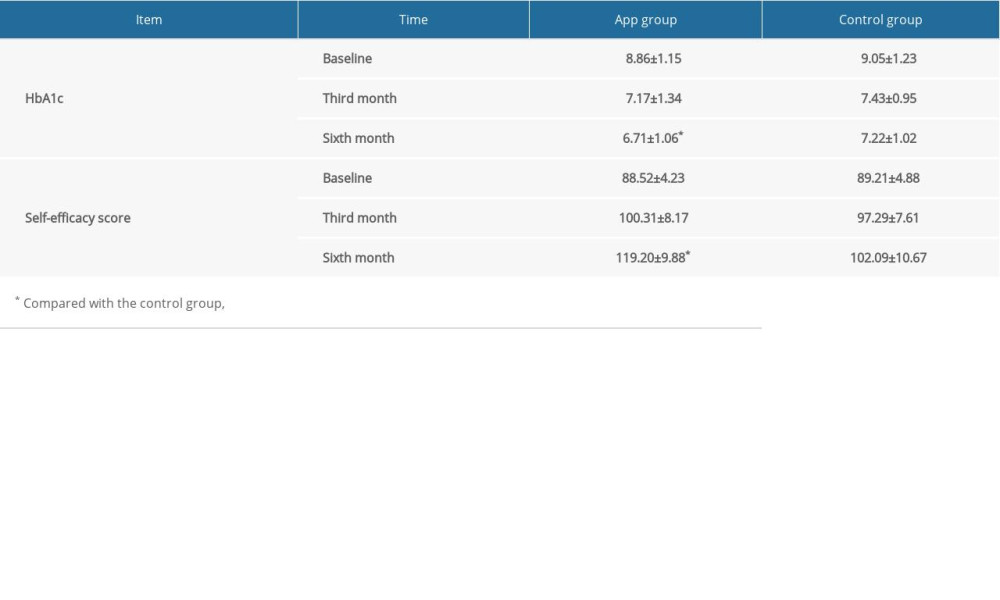
RESULTS: At the sixth month, patients in the app group showed better HbA1c control (6.71±1.06 vs. 7.22±1.02, P<0.05) and improved self-efficacy score (119.20±9.88 vs. 102.09±10.67, P<0.05).
CONCLUSIONS: The mobile app helped patients with type 2 diabetes in a community hospital improve therapeutic outcome and self-management behavior. It also provided experiences for prevention and management of other chronic diseases in community hospitals.
Keywords: Diabetes Mellitus, Type 2, Mobile Applications, Self Efficacy, Cohort Studies, Glycated Hemoglobin A, Hospitals, Community
Background
Type 2 diabetes is a common chronic disease affecting large numbers of people. By 2035, there will be 592 million people worldwide with diabetes [1]. A previous large-scale study showed that with the growth of the economy, improvement of life quality, changing lifestyle, and aging population, the prevalence of type 2 diabetes in China has reached 11.6%, and the prediabetes prevalence rate is 50.1%. However, the blood glucose control rate (hemoblobin A1c [HbA1c] <7%) was only 39.7% [2]. Diabetes and its complications not only seriously affect people’s health, but also bring huge economic burdens to families and society. Because diabetes is a chronic disease, developed countries have carried out various research projects to evaluate the effectiveness of community chronic disease prevention and treatment since the 1990s, the results of which were remarkable, especially in improving the capabilities of medical personnel in community hospitals [3–6]. In recent years, Chinese health administrative agencies have gradually realized the importance of conducting prevention and treatment of chronic diseases in community hospitals. Therefore, the government is promoting a graded diagnosis and treatment system to ease the pressure on large hospitals. At present, China has an enormous number of diabetic patients and the consequent health care burden; therefore, local governments have emphasized the positive role of community clinics and family doctors in managing chronic diseases. However, the growing diabetic population and the accompanying complications and psychological problems still pose great challenges to doctors.
In the 1960s, with the expansion of modern communication and internet technologies, the concept of telemedicine emerged [7]. Mobile medicine, part of telemedicine, refers to the use of small, portable computing or communication instruments that can be carried around to transmit health care information for health care providers or patients and has been widely used since 2003 [8]. Currently, mobile medicine is mainly applied by mobile phones. With the aging of the global society and the changes of demographic structure, there is a greater demand for medical services for the elderly. Traditional hospital services are unable to provide long-term management of chronic diseases in the elderly and other individuals. As a result, combined efforts of families and communities are needed to provide health care and disease prevention. In diabetes management, some mobile phone applications (apps) can help doctors understand the patient’s blood sugar status, adjust the patient’s lifestyle, improve blood sugar control, optimize the patient’s treatment regimen, and perform individualized diabetes management, thereby reducing medical expenses. For hospitals, patients, and medical insurance, these apps have enormous potential benefits. Few studies have evaluated the effect of a mobile app on glycemic control and self-efficacy in type 2 diabetes mellitus (T2DM) at a community hospital.
Our study aimed to observe the impact of the mobile phone diabetes management app (Yutangyihu) on HbA1c and self-efficacy in community hospital-diagnosed type 2 diabetes patients on the basis of conventional therapy.
Material and Methods
TRIAL DESIGN:
The approval of the Tianjin Medical University Ethics Board was obtained and the study was conducted according to the Declaration of Helsinki. All patients involved in our study signed informed consent forms. This trial was registered with the Chinese Clinical Trail Registry (no. ChiCTR2000034963).
This study was a single-center, open-label, prospective randomized controlled trial. Eligible patients were recruited by qualified physicians in the outpatient department of Zhangjiawo Community Health Service Center. The allocation ratio was 1: 1, and patients were equally divided into the mobile app group and the control group.
SAMPLING:
Recruitment and grouping of patients: (1) A telephone invitation conducted by a public health doctor of the Zhangjiawo Community Health Service Center. A total of 400 patients with type 2 diabetes registered in the center was called, of which 160 patients volunteered to participate our project. According to the inclusion and exclusion criteria, 40 patients were excluded. One-hundred twenty subjects who met the criteria were selected and randomly divided into the mobile app group (n=60) and the control group (n=60). The app group had access to the mobile app during routine clinical care from December 2018 to June 2019.
INCLUSION CRITERIA:
(1) Patients with type 2 diabetes diagnosed according to the Diagnostic Criteria for Type 2 Diabetes developed by the World Health Organization in 1999 on the basis of medical records; (2) diagnosed with diabetes ≥3 months; (3) age between 18 and 60 years; (4) no plans to relocate and travel in the next 6 months; (5) cellphone users.
EXCLUSION CRITERIA:
(1) Serious complications with kidney, eye, foot, and nervous system and acute complications such as diabetic ketoacidosis or lactic acidosis; (2) cognitive impairment, severe hearing and visual impairment; (3) type 1 diabetes or other unusual types of diabetes; (4) pregnancy and malignant tumors; (5) physically disabled; (6) surgery, pregnancy, and breastfeeding in the past 3 months; (7) patients who are participating in similar studies.
DEMOGRAPHICS:
(1) General data survey: gender, age, education level, marital status, personal income, and medical expenses. (2) Medical history data: duration of diabetes, complications of diabetes, other chronic diseases (e.g., hypertension, coronary heart disease, stroke, hyperlipidemia, tumors).
END POINTS: (1) Metabolic index: glycated hemoglobin (HbA1c). (2) Diabetes Self-Efficacy Rating Scale (DSES) [9,10] score: This scale was compiled by Hurley and Shea [10], translated and revised by Professor Wong into Chinese [9]. The scale has been reported to have good reliability and validity [11]. It consists of 6 dimensions and 26 items: self-efficiency on diet (6 items), regular exercise (4 items), medication (3 items), blood glucose monitoring (4 items), foot care (5 items), and prevention and management of high and low blood glucose (4 items), which was scored by the Likert 5 Grade method, with a total score ranging from 26 to 130. The higher the score, the better the patient’s self-efficacy.
METHODS:
The diabetes health care management platform “YuTangYiHu” app was developed by Beijing Aihe Health Technology Co. Ltd. The app could synchronically read glucose values by a cellphone cable-connected glucometer and provide support for diabetes self-management by diet advice, emotional management, and medication guidance. The 60 patients of the app group were trained to use the mobile app during a routinely scheduled clinic visit by a physician or diabetes educator. The training was carried out for 2 h/week for 3 weeks. The training covers app installation, monitoring blood glucose by the provided glucometer device, and communication with physicians and educators. All patients were required to test HbA1c and evaluate self-efficacy by the DSES questionnaire when enrolled and at the third month and the sixth month.
Blood glucose data were compiled into charts in the doctor’s version of the Yutangyihu app and subsequently viewed by the outpatient doctor. The education nurse provided online instruction available to patients every night from 2: 00 PM to 6: 00 PM, including giving instructions about diet, exercise, blood glucose monitoring, insulin injection, and answering patients’ questions. When the patient uploaded an abnormal blood glucose result, they analyzed the causative factors and gave advice on how to avoid them.
STATISTICAL ANALYSIS:
The database was built and statistical analysis was performed by SPSS 17.0 software. Measurement data are expressed as mean±standard deviation. Statistical methods included
Results
COHORT CHARACTERISTICS:
Two patients of the control group withdrew from the trial (one moved out of the city and the other due to the loss of contact). The control group was 58 cases with a loss rate of 1.4%. The loss did not affect the results of the study, and the cause of loss was not related to the study. Among the patients surveyed, men made up 66.2%. The ages ranged from 47 to 60 years, with an average age of 55.64±14.2, of which 41 patients were ≥50 years, accounting for 90.2%. There were no significant differences in age, education level, duration of diabetes, fasting or postprandial plasma glucose, triglyceride, low-density lipoprotein, and urine albumin/creatine ratio between the 2 groups when enrolled (P>0.05) (Table 1).
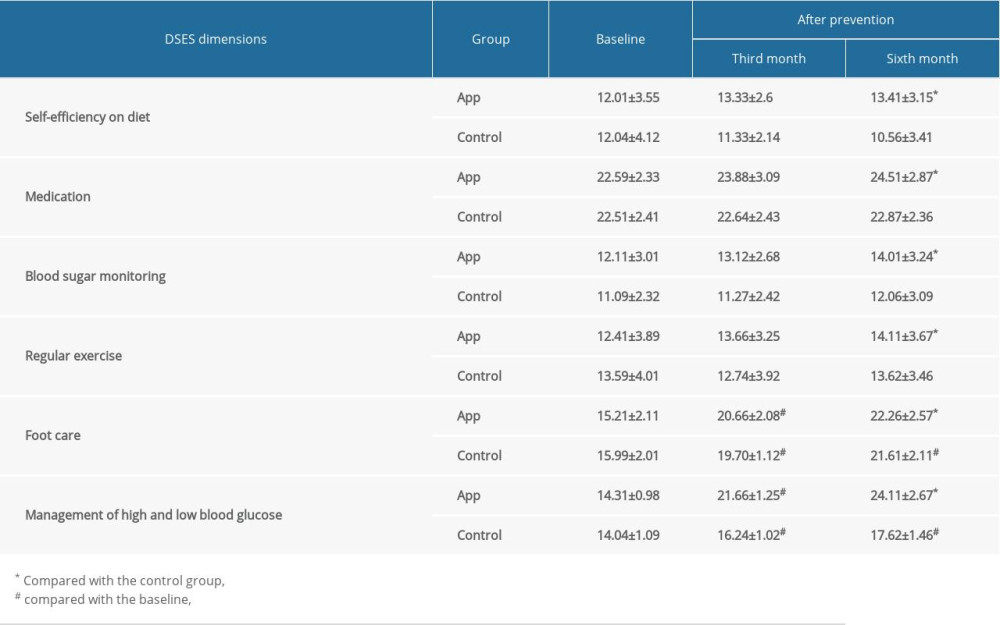
The total scores of self-efficacy are shown in Table 2. After 6 months, the total score of self-efficacy was 119.20±9.88 for the app group and 102.09±10.67 for the control group (P<0.05). For the 6 dimensions of DSES, the self-efficacy scores are shown in Table 3. After 3 or 6 months of intervention, although the patients in the control group had a significant improvement in the self-efficacy total score from the baseline, including the dimensions of foot care and the management of high and low blood glucose (P<0.05), patients in the app group performed better in all 6 dimensions after 6 months (P<0.05).
Our study evaluated the intervention effect by HbA1c, a criterion standard for management effects of T2DM by clinical guidelines. There was no significant difference in HbA1c between the 2 groups at baseline and at the third month of treatment (Table 2). After the intervention with the mobile app for 6 months, the HbA1c in the app group decreased significantly compared with the control group (P<0.05).
Discussion
China faces a growing population with chronic diseases, especially diabetes and its complications [2]. In recent years, local governments have emphasized the positive role of community management in chronic diseases. With new effective diabetes treatment techniques being explored, it is important to strengthen patients’ health education and behavioral support. Some studies have pointed out that self-management of diabetic patients is the basis of all diabetes management [12]. The improvement of nursing knowledge and skills alone did not guarantee that patients could perform good self-care. Patients’ ability to judge whether they can perform a certain self-care behavior, or self-efficacy, was more meaningful for diabetes management.
In this study, we used the app to assist diabetes management. It included data visualizations designed to help with the identification of patterns in blood glucose, insulin, carbohydrate, and exercise data. The data were shared from the software to a cloud data management system to facilitate review by the medical staff.
Cohort characteristics (Table 1) showed that most of the diabetic patients in this community hospital are middle-aged and senior citizens, with an average age of 55.64±14.2 years; 21.1% of the app group and 18.5% of the control group received a high school education and above. Most type 2 diabetes patients in this community were less educated and had greater needs to have access to the mobile app to manage diabetes.Table 3 shows that at baseline the self-efficacy score of all patients was higher in the dimension of medication (22.59±2.33
The role of behavioral change in diabetes management has drawn more attention and is now a sign of the success of diabetes education [14]. Regular guidance and supervision by caregivers could enhance patients’ self-efficacy. Under community management, the mobile app intervention could enhance the interaction between medical staff and patients and replace patients’ visits to some extent. Our staff in the community hospital assessed patients’ eating habits, made individualized exercise programs, and urged the change of unhealthy lifestyles so that they can acquire relevant knowledge and skills and improve self-efficacy scores in the dimensions of diet, regular exercise, and management of high and low blood sugar.
Mobile medical technology supports clinical treatment and health management mainly through intelligent application, which helps doctors better understand the daily blood glucose levels of patients and provides timely guidance to perform individualized diabetes management and improve the efficiency of disease management [15]. Previous studies showed that use of diabetic mobile apps were closely related to the improvement of patient self-efficacy and metabolic indicators. Use of the app intervention optimized medical resources and increased the time for patient education [15,16]. It relies on clinicians and education nurses to carry out special training for enrolled patients to improve their knowledge and diabetes self-management ability [16]. Blood glucose monitoring and individualized treatment using the app could effectively increase the patient’s self-confidence and skills in dealing with diabetic complications and dangerous events, which could prevent the occurrence of complications and improve the quality of life. This was confirmed by higher patient self-efficacy scores in “treatment of high and low blood glucose events” after the app intervention. Compared with traditional education in hospitals, the mobile app is more flexible and feasible. In our study, the app group was evaluated by individualized dietary caloric index assessment and exercise volume analysis to assess the intervention effect. The high follow-up rate of the app group showed good compliance and satisfaction of patients with this form of management.
This study evaluated the effects of app intervention by testing patients’ HbA1c, which is the criterion standard for the diagnosis of diabetes. HbA1c reflects the average concentration of blood glucose of the previous 2–3 months. After the HbA1c value exceeded the high limit (HbA1c=7.0%), each 1% increase increases the risk of retinopathy by 33% [1]. The longer the duration, the greater the risk. Therefore, effective control of HbA1c is critical for patients’ prognoses. On the basis of clinical treatment, compared with the control group, there was no statistically significant difference in HbA1c between the 2 groups after 3 months (Table 2). However, the HbA1c of the app group was significantly lower than that in the control group at the sixth month. Patients’ improvement from knowledge of the disease to self-management behavior took a long time. In this study, patients’ behavioral changes occurred before the metabolic index changes. This was why HbA1c improvement is not obvious at the third month. Most of the patients (50.0%) had a junior high school education level, which led to certain difficulties in the use of smart phones. The patients’ proficiency in using the software also affected the blood glucose values for the first 3 months.
Our study included a small but reasonably sized and diverse sample of community hospital patients who were introduced to the mobile app. The limitations of our study included lack of separation of the patients into insulin and noninsulin groups and not fully analyzing the characteristics of app use. After interviewing the patients, the most commonly used app functionality was for blood glucose recording and for tracking meal and carbohydrate intakes. The majority of the respondents reported that the app was very easy to navigate. The follow-up period was short and data on diet, exercise, and lifestyle change were not available, which might introduce bias into the results of glycemic control.
Conclusions
In conclusion, on the basis of routine clinical visits, the diabetes app intervention has helped patients with type 2 diabetes to improve clinical treatment and self-management behavior. As a result, mobile app interventions in community hospitals might be applied to improve the control of other chronic diseases and achieve better clinical outcomes.

References
1. Cho NH, Shaw JE, Karuranga S, IDF diabetes atlas: Global estimates of diabetes prevalence for 2017 and projections for 2045: Diabetes Res Clin Prac, 2018; 138; 271-81
2. Xu Y, Wang L, He J, Prevalence and control of diabetes in Chinese adults: JAMA, 2013; 310(9); 948-58
3. Hayes JT, Boucher JL, Pronk NP, The role of the certified diabetes educator in telephone counseling: Diabetes Educ, 2001; 27(3); 377-86
4. Valdez GM, Dadich KA, Boswell C, Planning and implementing an interdisciplinary diabetes workshop for healthcare professionals: J Contin Educ Nurs, 2007; 38(5); 232-37
5. Andersson CM, Bjärås Gunilla EM, Östenson C–G, A stage model for assessing a community-based diabetes prevention program in Sweden: Health Promot Int, 2002; 17(4); 317-27
6. White J, White paper on the prevention of type 2 diabetes and the role of the diabetes educator
7. Hersh WR, Patterson PK, Kraemer DF, Telehealth: J Am Med Inform Assoc, 2002; 9(1); 89-91
8. Bellini P, Bruno I, Cenni D, Mobile medicine: Semantic computing management for health care applications on desktop and mobile devices: Multimed Tools Appl, 2012; 58(1); 41-79
9. Wong C, Lam C, Lo Y: Confirmatory factor analysis on traditional Chinese version of 26-item Diabetes Self-Efficacy Scale (C-DSES) in Chinese patients with type 2 diabetes mellitus, 2011, University of Hong Kong
10. Hurley AC, Shea CA, Self-efficacy: Strategy for enhancing diabetes self-care: Diabetes Educ, 1992; 18; 146-50
11. Anderson RT, Balkrishnan R, Camacho F, Patient-centered outcomes of diabetes self-care. Associations with satisfaction and general health in a community clinic setting: N C Med J, 2003; 64(2); 58-65
12. Duncancarnesciali J, Wallace BC, Odlum M, An evaluation of a diabetes self-management education (DSME) intervention delivered using avatar-based technology: Certified diabetes educators’ ratings and perceptions: Diabetes Educ, 2018; 44(3); 216-24
13. Jeng C, Braun LT, Bandura’s self-efficacy theory: J Hol Nurs, 1994; 12(4); 425-36
14. Chatterjee S, Davies MJ, Stribling B, Real-world evaluation of the DESMOND type 2 diabetes education and self-management programme: Pract Diabetes, 2018; 35(1); 19-22a
15. Bene BA, O’Connor S, Mastellos N, Impact of mobile health applications on self-management in patients with type 2 diabetes mellitus: Protocol of a systematic review: BMJ Open, 2019; 9(6); e025714
16. Desveaux L, Shaw J, Saragosa M, A mobile app to improve self-management of individuals with type 2 diabetes: Qualitative realist evaluation: J Med Internet Res, 2018; 20(3); e81
In Press
Clinical Research
Effect of Low-Dose Vonoprazan on Hepatic Cytochrome P450 Activity By 13C-Aminopyrine Breath Test in Healthy...Med Sci Monit In Press; DOI: 10.12659/MSM.953332
Database Analysis
COVID-19 and Diabetes: Clinical Symptoms, Acute Kidney Injury, Inflammatory Response, and Poor Prognosis Fa...Med Sci Monit In Press; DOI: 10.12659/MSM.951864
Clinical Research
Comparative Effectiveness of a Nurse-Led Care Model vs Usual Care in Rheumatoid Arthritis: A Longitudinal C...Med Sci Monit In Press; DOI: 10.12659/MSM.953211
Clinical Research
Impact of Treatment Modality on Pain, Sexual Function, and Psychological Well-Being in Patients With Bartho...Med Sci Monit In Press; DOI: 10.12659/MSM.952422
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,007
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,757,384
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,095
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,748
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387