25 June 2021: Clinical Research
Intervals and Outcomes of First and Second Pregnancies in Low-Income Women: A Record-Linkage Longitudinal Prospective Cohort Study
David C. Reardon1ABCDEFG*, Christopher Craver2ACDEDOI: 10.12659/MSM.931596
Med Sci Monit 2021; 27:e931596






Abstract
BACKGROUND: The number of pregnancies and interval between pregnancies can have significant impact on a woman’s reproductive, psychological, and general health. Exposure to multiple reproductive losses is especially associated with higher rates of negative outcomes.
MATERIAL AND METHODS: Medical records from 1999-2012 for all Medicaid beneficiaries born after 1982 in the 17 states that provide coverage for all reproductive services (N=2 162 600) were examined to identify the timing of subsequent pregnancies and their outcomes within 3 years of a first known pregnancy.
RESULTS: One year after their first pregnancy outcomes, 22.6%, 17.8%, and 11.7% of women who had an induced abortion, a natural loss, or a birth, respectively, conceived at least 1 additional pregnancy. By the second year, the percentage of repeat pregnancies rose to 37.5% after an abortion, 25.6% after a natural loss, and 23.1% after a birth. Graphing the weekly conception rates revealed that women who had abortions and natural losses showed similar patterns of rapid repeat pregnancy, with the rate of second conception spiking quickly within 3 to 4 months after the first pregnancy outcome.
CONCLUSIONS: These findings support the clinical evidence that pregnancy loss may contribute to rapid repeat pregnancies and may better inform interventions to reduce rapid repeat pregnancies.
Keywords: Birth Intervals, Birth Rate, Epidemiologic Studies, reproductive health, Cohort Studies, Gravidity, Longitudinal Studies, Medicaid, Poverty, Pregnancy, Pregnancy Outcome, Prospective Studies, Time Factors, United States
Background
Interpregnancy pregnancy intervals (IPI) are an important public health concern in relation to health outcomes for subsequent pregnancies. There is good evidence that better perinatal outcomes are likely when there is 18 to 23 months between deliveries [1,2]. For example, pregnancies conceived within 5 months of a delivery are associated with third-trimester bleeding, premature rupture of membranes, puerperal endometritis, anemia, and maternal death [1]. There is not good evidence, however, regarding the optimum IPI for a delivery following a pregnancy loss. A recent literature review of deliveries following miscarriage found that delaying pregnancy for 6 months following miscarriage does not significantly improve subsequent pregnancy outcomes [3]. Regarding the optimum IPI for a delivery following induced abortion, we could not find any evidence-based medical findings.
The desire for a replacement pregnancy following a pregnancy loss (natural or induced) may contribute to short pregnancy intervals, known as rapid repeat pregnancies [4], generally defined as a pregnancy within 12 to 24 months of a previous pregnancy. For women who experience a natural loss, a desire for a replacement pregnancy is common and a subsequent live birth may be emotionally healing relative to feelings of grief and self-blame associated with the previous loss [5]. Similar desires may arise following an abortion, especially when certain risk factors are present, such as feeling pressured by male partners or parents to undergo an unwanted abortion, or there is a high level of attachment to the pregnancy, ambivalence, or moral conflict surrounding the abortion decision [6]. In a survey of women who had sought post-abortion counseling, 29% reported seeking replacement pregnancy [7]. In another study of metropolitan teens who terminated a first pregnancy, 27% had a second pregnancy within 12 months, 49.8% within 18 months, and 74.9% within 24 months [8]. Another study of young women (aged 13–21) seeking prenatal care reported that 44% had become pregnant again within 12 months of a prior pregnancy outcome [9]. While the authors of that study reported that rapid repeat pregnancies were less common following a delivery, they did not provide details regarding any differences between spontaneous and induced abortions.
Motivated by the observations above, we hypothesized that the rates of rapid repeat pregnancy (within 24 months of the previous pregnancy) are higher following both natural losses and induced abortion. The purpose of this study was to examine the incidence rate and outcome of second pregnancies and third pregnancies within 3 years of a first pregnancy outcome within a large population of young, low-income women in the United States.
Material and Methods
Data were obtained from the Centers for Medicare and Medicaid Services (CMS) from the 17 states (Alaska, Arizona, California, Connecticut, Hawaii, Illinois, Maryland, Massachusetts, Minnesota, Montana, New Jersey, New Mexico, New York, Oregon, Vermont, Washington, and West Virginia) where Medicaid includes coverage of all reproductive health care options, including induced abortion, covering the years 1999 through at least 2012, inclusive. The study population was limited to all women born in 1983 or later and had been eligible for Medicaid coverage for at least 12 months between 1999 and 2012. Data collection began in the year women turned 14 years of age. The subsample used for this analysis consisted of all Medicaid beneficiaries over the age of 13 between 1999 and 2009, inclusive, for whom their data indicated at least 1 identifiable pregnancy outcome (using ICD-9 codes 630–679, V22, V23, V27). The first identified pregnancy outcome was treated as the index pregnancy, and the next two pregnancy outcomes (if any) within the three years following the index pregnancy were identified to examine the pattern of up to three pregnancy outcomes and the pregnancy interval between the index and second pregnancies. Once a woman was identified as having a pregnancy outcome, her beneficiary code was used to link her records to Medicaid coverage in any state in which she had subsequent coverage in order to account for any changes of address. By restricting our search for the index pregnancy to 2009, we allowed for 3 years of follow-up on women whose index pregnancy was in 2009. The oldest women in 2009 would have been 26 while the youngest would have been 14. Since Medicaid eligibility is limited to only individuals and households who meet low-income requirements, the sample is limited to low-income women.
Pregnancy outcomes were identified using both diagnostic ICD codes and CPT/HCPS treatment codes (01964; 01965; 01966; 59100; 59120; 59121; 59130; 59135; 59136; 59140; 59150; 59151; 59320; 59325; 59812; 59820; 59821; 59830; 59840; 59841; 59850; 59851; 59852; 59855; 59856; 59857; 59866; 59866; 81025; 84163; 88304; 88305; 0502F; X7724; X7726; Z0336; S2260; S2265; S2266; S2267; S0199; S8055). Multiple diagnostic or treatment codes for any pregnancy within 30 days of other pregnancy codes were collapsed into a single pregnancy outcome using the first date associated with that cluster of Medicaid claims.
The first known pregnancy outcome for each beneficiary was marked as that woman’s index pregnancy. Following the index pregnancy, we identified the outcome of any subsequent pregnancy within 3 years (156 weeks) of the date of the index pregnancy outcome. Pregnancy outcomes were segregated into 3 categories: live birth; induced abortion; natural fetal loss (miscarriage, ectopic pregnancy, molar pregnancy, or still birth). Since the classifications for missed abortion (ICD 632; N=28,859), unspecified abortion (ICD 637; N=12,655), and failed attempted abortion (ICD 638; N=0) are sometimes used to encompass both induced and spontaneous abortions, women with these outcomes were excluded to avoid introducing the ambiguities associated with these overlapping classifications. Similarly, the small number of women identified as having had an illegally induced abortion (ICD 636; N=271) were excluded since these cases might be significantly different than legally induced abortions. Twins and other multiple pregnancies resulting in a combination of both live birth and fetal loss (N=0) were also excluded. Neonatal deaths were not identifiable. Also, to address coding errors or other conflicts with the data, coding indicating an induced abortion within 36 weeks prior to a live birth was excluded, as well as any data indicating an abortion or natural loss within 4 weeks of an abortion.
For the analysis of the pregnancy interval between the first and second pregnancy, we calculated the weeks between the index pregnancy outcome date and the estimated date of conception relative to the second pregnancy outcome and date. If the second pregnancy outcome was a live birth, we deducted 40 weeks from the second pregnancy outcome date and designated that week as the estimated conception date. If the second pregnancy outcome was an abortion, we deducted 8 weeks. For natural losses, we deducted 12 weeks based on the assumption that early miscarriages are less likely to be treated and, therefore, the treated miscarriages in this population are, on average, more likely to be later in gestation than elective abortions.
To explore potential differences between beneficiaries whose first pregnancy occurred when they were teenagers to those who were 20 to 26 years of age, pregnancy pattern and pregnancy interval tables were also created for each age group. Summary analytic tables were created using (SAS/STAT) software, version 10 of the SAS System for Unix. All comparative analyses and graphs were completed using Microsoft Office Excel.
The ethics of the study design was reviewed and approved by the Sterling Institutional Review Board. No patients were involved and informed consent was not required. Anonymized data were provided by the United States Centers for Medicare and Medicaid Services under strict conditions securing the privacy of patient records.
Results
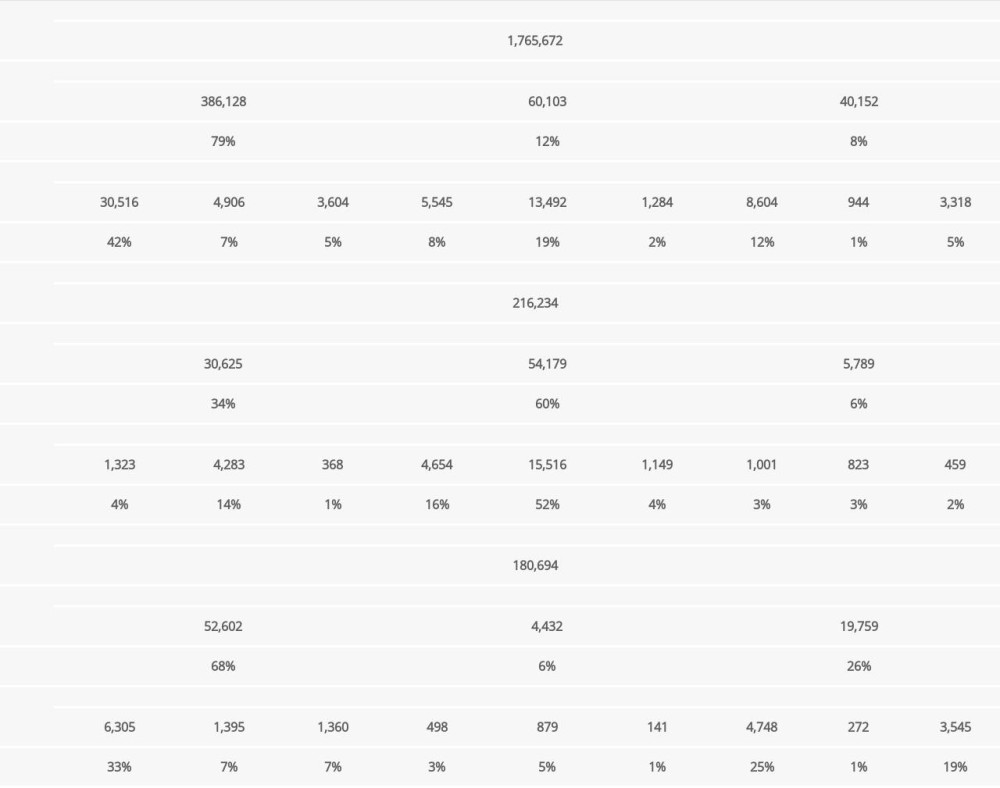
In the cohort described above, a total of 2 162 600 young Medicaid beneficiaries had at least 1 pregnancy outcome between 1999 and 2009, inclusive. Table 1 shows the distribution of the first 3 pregnancies among the study population. Within 3 years of their index pregnancy, 30.2% of beneficiaries had at least 1 additional pregnancy outcome and 5.6% had two or more additional pregnancy outcomes. Among beneficiaries with a natural loss (180 694), 42.5% had a second pregnancy outcome, and 10.6% had two or more within the three years examined. These rates were very similar to those of women whose first pregnancy was aborted (216 234), with 41.9% having at least 1 additional pregnancy, and 13.7% having two or more pregnancies within the 3-year window. While the number of subsequent pregnancies was very similar for women who had abortions and natural losses, the women who had previously aborted were much more likely to have another abortion (60% versus 6%), while women who had a natural loss were much more likely to have another natural loss (26% versus 6%), or a live birth (68% versus 34%).
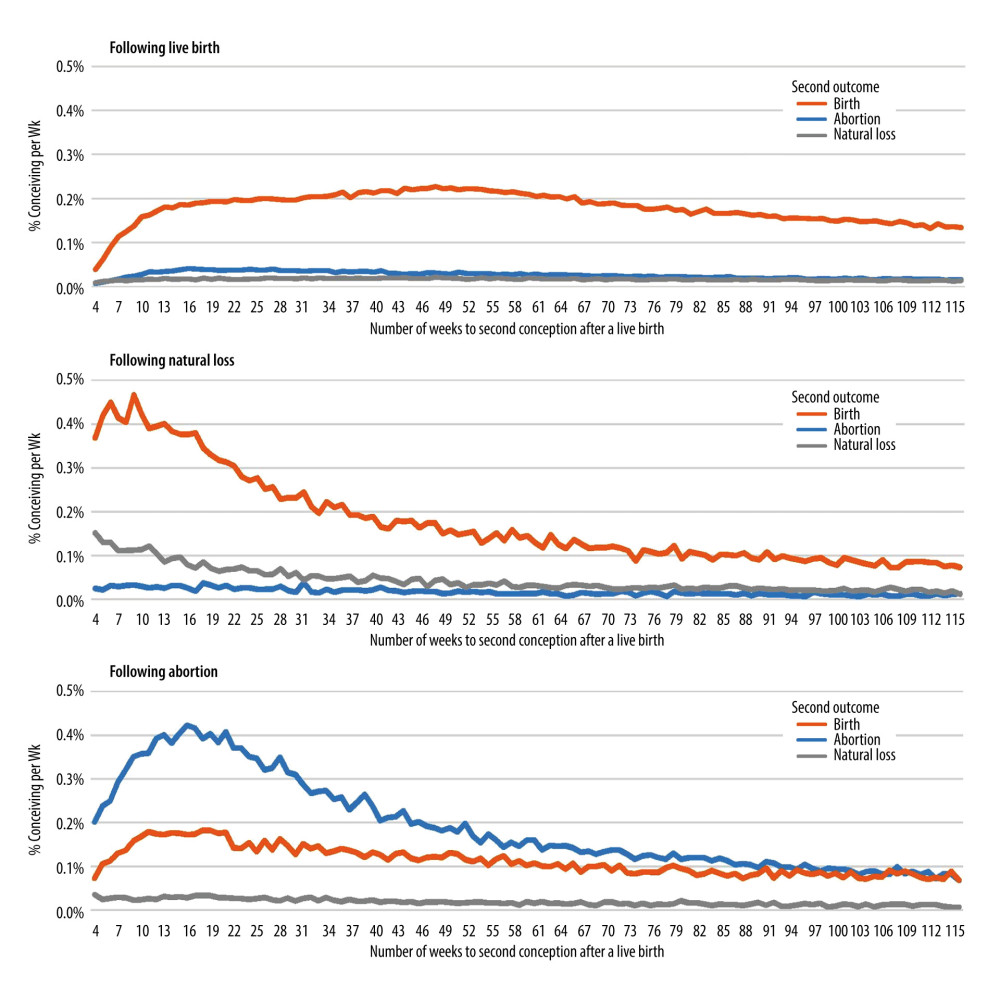
Figure 1 shows the interval in weeks following each index pregnancy outcome until the estimated conception date of the second pregnancy segregated according to the second pregnancy outcome. The y-axis indicates the percentage of women with the first outcome who conceived a pregnancy in approximately the week indicated by the x-axis. The x-axis was limited to 116 weeks (3 years minus 40 weeks for a live birth), which was sufficient to include the full range of conception dates for women giving birth. Figure 1 shows that the conception rates following pregnancy loss (abortion or natural loss) were more than double the conception rate following a live birth during the first half year. Moreover, the conception rate following a live birth was relatively flat, approximately 0.2% per week for the first year following a delivery, whereas the rates following a natural loss or abortion rose rapidly to 0.5% per week or more (all outcomes combined) and remained elevated for approximately 1 full year before reaching a plateau.
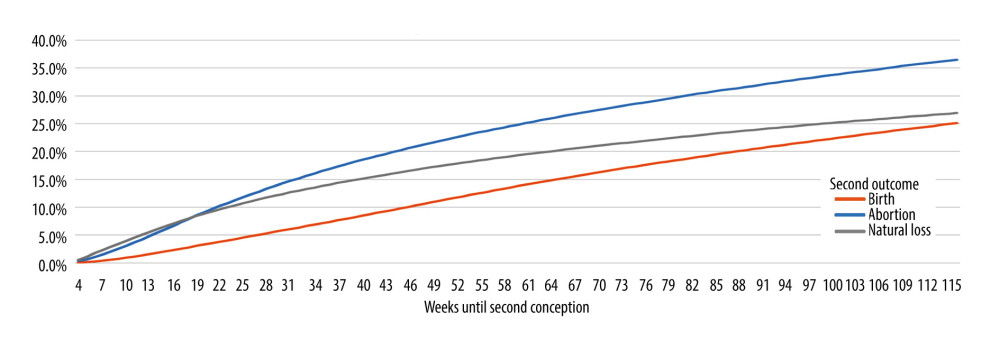
The heightened rates of conception following a pregnancy loss are further illustrated in Figure 2, which shows the cumulative percentage of women pregnant at each week following either a live birth, abortion, or natural loss. One year after their first pregnancy outcome, 22.6%, 17.8%, and 11.7% of women who had an abortion, a natural loss, or a birth, respectively, had conceived at least 1 additional pregnancy. These percentages rose to 34.5%, 25.6%, and 23.1%, respectively, by the end of two years and to 46.5%, 45.2%, and 27.4%, respectively, at the end of 3 years.
Additional analyses were performed to compare women whose first pregnancy outcomes were before the age of 20 compared to the older beneficiaries. The results revealed that pregnancy and interval patterns were very similar for both age groups. The most significant difference was that among women who aborted their first pregnancy, teens were moderately more likely to carry their second to term than were older women. Complete tables and figures comparing these two age groups are included in the Supplementary Material (Supplementary Figures 1–3 and Supplementary Tables 1, 2).
Discussion
The average interval between a first pregnancy outcome and conception of a second pregnancy is shorter following a pregnancy loss of any type than for women who deliver. Moreover, the rate of rapid repeat pregnancies, measured as a cumulative percentage, is very similar for both natural losses and abortions for approximately the first 6 months following the loss and is higher thereafter for abortion. This pattern is consistent with the hypothesis that pregnancy losses of all types are associated with replacement pregnancies [4,7–9]. It is noteworthy, however, that while some women becoming pregnant soon after an abortion will carry to term, and the percentage having a second abortion is higher than the number giving birth. This finding, however, is also consistent with self-reports and clinical evidence indicating that the problems existing at the time of a first abortion, especially pressure and coercion from other people, are likely to still exist at the time of the second abortion [7]. In addition, there is some evidence that for some subset of women, rapid repeat abortions may involve aspects of self-punishing behavior, which has been reported to include substance abuse, promiscuity, self-harm, recklessness, suicidal behaviors, and repetitive abortions even in anticipation of additional regret or self-hate [7,10]. In this light, rapid repeat abortions are not necessarily indicative of abortion being used as a substitute for birth control, but may instead be indicative of the prevalence of coercion and/or conflicting and ambivalent desires for a pregnancy under circumstances that are less than ideal [6]. Our findings are also consistent with the results of an analysis from Scotland that revealed a higher rate of live births for second pregnancies conceived within 6 months of a miscarriage [11].
This study is unique in identifying pregnancy patterns and pregnancy intervals following induced abortion. The finding that 22.6% of women who abort are pregnant again within 1 year, and 37.5% are pregnant again within two years, is consistent with the evidence that a substantial portion of abortions are unwanted (the result of some level of coercion) or may otherwise trigger a desire for replacement pregnancies in some women [7]. While a disproportionate number of second pregnancies were also aborted, this is most likely due to a continuation of circumstances (such as pressure from others, scant economic resources, and limited job and education alternatives) that make the continuation of even wanted pregnancies difficult. This suggests that women seeking abortions should be carefully screened for any feelings of attachment to the pregnancy, or any preference for giving birth “if I was supported by others” or “if I was in better circumstances” [6]. In such cases, it is likely that the abortion is not being sought to advance the woman’s own self-interests, but rather to satisfy the demands of others or circumstances when she would really prefer to be empowered to give birth to her child. It is likely that these cases of unwanted abortions account for a significant portion of the increased risk of psychological disorders associated with abortion [6,12], including elevated rates of postpartum psychiatric illness [13].
A number of limitations apply to this study. First, the available data were limited to young low-income women. Additional research is necessary to see if the trend in differences observed here also applies to middle- and upper-income classes. Second, Medicaid eligibility changes with age, circumstance, across states, and across different fiscal years. The identification of pregnancy events is therefore not complete. Third, for many beneficiaries, the calculated estimate for the week of conception could be off by several weeks, especially in cases of late natural losses or very premature births, but neither the second or third limitation are likely, individually or together, to alter the general trend shown in our findings.
Finally, the most significant limitation is that there is no direct information relative to any intentionality associated with any of these conceptions. It is well known that a substantial portion of both delivered and miscarried pregnancies are unplanned. In some cases, the natural loss of an unplanned pregnancy may be experienced with more relief than feelings of loss. Conversely, induced abortions are not limited to only unwanted pregnancies. A review of the literature reveals that the percentage of abortion patients describing their pregnancy as wanted or meaningful ranges from as low as 11% to as high as 63% [6]. A more recent study has reported that only 42% of women receiving induced abortions identify the pregnancy as unwanted [14]. Therefore, without survey data regarding the intentionality of and/or emotional attachment to these pregnancies, our findings cannot distinguish between intentional replacement pregnancies, unconsciously desired replacement pregnancies, contraceptive failures, or lack of contraceptive use. Despite this important limitation, the similarity in IPI rates following spontaneous and induced abortions supports the hypothesis that these two groups have overlapping similarities. In addition, while these findings do not measure intention, they are consistent with what would be expected if the self-reports of women who report replacement pregnancies following a pregnancy loss [7] are common enough to be observable in a population study.
Given the above limitations, confidence in our findings relative to first-pregnancy outcomes was strengthened by our decision to limit the cohort to younger women, specifically those born after 1982. In the first year of data, 1999, the oldest beneficiaries included in our data were 16 years of age. In addition, the study population was limited to women who had at least 12 months of eligibility for Medicaid coverage between 1999 and 2012, inclusive. This second limitation excluded the most transitional beneficiaries, such as teenagers from middle- and upper-income families, who were only temporarily eligible for Medicaid because of their pregnancy and desire for a Medicaid-funded abortion. The resulting sample represents women who were most likely eligible for at least their first pregnancy and had significant eligibility in the months and years following that index event.
Conclusions
Our findings show that there are similarities in the elevated risk of a rapid repeat pregnancy following either a natural pregnancy loss or an abortion. In the absence of direct information regarding pregnancy intention, these results do not provide any direct measure of the incidence rate of replacement pregnancies. These findings should inform future research on interpregnancy intervals and motivate efforts to provide interventions, such as contraception and loss counseling, that may reduce rapid repeat pregnancies and any associated sequelae [15].
Supplementary Material
Supplementary Analyses
SUPPLEMENTARY ANALYSES:
The following shows comparisons made between Medicaid beneficaries whose first pregnancy was before the age of 20 and women whose first pregnancy was between the ages of 20 and 26. There were two reasons for this comparison. First, there may be significant differences between teenagers and older beneficiaries. Second, it is highly likely that Medicaid data is capturing the first pregnancy outcome for low-income teenagers since eligibility requirements are most easily met in all states for these youngest women.
These supplementary results include both the pregnancy interval patterns between the first and second known pregnancies and the pregnancy pattern trees for both groups.
The results show very similar patterns for both groups, with the one exception that teens who aborted their first pregnancy were somewhat more likely than older beneficiaries to carry their second pregnancy to term (37% to 31%).
References
1. Conde-Agudelo A, Belizán JM, Maternal morbidity and mortality associated with interpregnancy interval: Cross sectional study: BMJ, 2000; 321; 1255-59
2. Smith GCS, Pell JP, Dobbie R, Interpregnancy interval and risk of preterm birth and neonatal death: retrospective cohort study: BMJ, 2003; 327; 313
3. Kangatharan C, Labram S, Bhattacharya S, Interpregnancy interval following miscarriage and adverse pregnancy outcomes: Systematic review and meta-analysis: Hum Reprod Update, 2017; 23; 221-31
4. Horowitz NH, Adolescent mourning reactions to infant and fetal loss: Soc Casework, 1978; 59; 551-59
5. Smith T, Davidson W, Roberson K, Permission to love: Celebrating your rainbow baby after a reproductive loss: Int J Childbirth Educ, 2018; 33; 46-48
6. Reardon DC, The abortion and mental health controversy: A comprehensive literature review of common ground agreements, disagreements, actionable recommendations, and research opportunities: SAGE Open Med, 2018; 6; 205031211880762
7. Burke T, Reardon DC: Forbidden grief: The unspoken pain of abortion, 2007, Springfield IL, Acorn Books
8. Koenig MA, Zelnik M, Repeat pregnancies among metropolitan-area teenagers: 1971–1979: Fam Plann Perspect, 1982; 14; 341
9. Jacoby M, Gorenflo D, Black E, Rapid repeat pregnancy and experiences of interpersonal violence among low-income adolescents: Am J Prev Med, 1999; 16; 318-21
10. Coleman PK, Boswell K, Etzkorn K, Turnwald R, Women who suffered emotionally from abortion: A qualitative synthesis of their experiences: J Am Physicians Surg, 2017; 22; 113-18
11. Love ER, Bhattacharya S, Smith NC, Effect of interpregnancy interval on outcomes of pregnancy after miscarriage: Retrospective analysis of hospital episode statistics in Scotland: BMJ, 2010; 341; c3967
12. Sullins DP, Abortion, substance abuse and mental health in early adulthood: Thirteen-year longitudinal evidence from the United States: SAGE Open Med, 2016; 4; 11
13. Reardon DC, Craver C, Effects of pregnancy loss on subsequent postpartum mental health: A prospective longitudinal cohort study: Int J Environ Res Public Health, 2021; 18; 1-11
14. Biggs MA, Neilands TB, Kaller S, Developing and validating the Psychosocial Burden among people Seeking Abortion Scale (PB-SAS): PLoS One, 2020; 15; e0242463
15. Qasba NT, Stutsman JW, Weaver GE, Informing policy change: A study of rapid repeat pregnancy in adolescents to increase access to immediate postpartum contraception: J Women’s Heal, 2020; 29; 815-18
Figures
In Press
Clinical Research
Institutional and Regional Variations in Access to Clinical Trials and Next-Generation Sequencing in Turkis...Med Sci Monit In Press; DOI: 10.12659/MSM.951027
Clinical Research
Low-Intensity Blood Flow-Restricted Multi-Joint Exercise Improves Muscle Function in Patients With Patellof...Med Sci Monit In Press; DOI: 10.12659/MSM.950516
Review article
Musculoskeletal Ultrasound and MRI in the Evaluation of Chemotherapy-Induced Peripheral Neuropathy: A ReviewMed Sci Monit In Press; DOI: 10.12659/MSM.951283
Clinical Research
Sensory Processing, Dissociation, and Affective Symptoms in Misophonia: A Cross-Sectional Study of 35 AdultsMed Sci Monit In Press; DOI: 10.12659/MSM.950938
Most Viewed Current Articles
17 Jan 2024 : Review article 10,187,196
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,708,487
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,341,643
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 706,524
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387