14 September 2021: Database Analysis
Chest Radiological Findings and Clinical Characteristics of Laboratory-Confirmed COVID-19 Patients from Saudi Arabia
Rowa Aljondi1ABCDE*, Salem Alghamdi1ABCDE, Abdulrahman Tajaldeen2ABCDE, Ikhlas Abdelaziz1BE, Lubna Bushara1AE, Hind A. Alghamdi3F, Hassan Alhinishi4B, Bandar Alharbi5B, Raied Alshehri5B, Abdullah Aljehani4D, Mansour Almotairi6BDOI: 10.12659/MSM.932441
Med Sci Monit 2021; 27:e932441






Abstract
BACKGROUND: Coronavirus disease 2019 (COVID-19) is a viral respiratory disease that first emerged in China in December 2019 and quickly spread worldwide. As the prevalence of COVID-19 increases, radiological examination is becoming an essential diagnostic tool for identifying and managing the disease’s progression. Therefore, we aimed to identify the chest imaging features and clinical characteristics of patients with laboratory-confirmed COVID-19 in Saudi Arabia.
MATERIAL AND METHODS: In this retrospective study, data of laboratory-confirmed COVID-19 patients were collected from 4 hospitals in Jeddah, Saudi Arabia. Their common clinical characteristics, as well as imaging features of chest X-rays and computed tomography (CT) images, were analyzed.
RESULTS: A total of 297 patients with laboratory-confirmed COVID-19 who underwent chest imaging were investigated in this study. Of these patients, 77.9% were male and 22.2% were female. Their mean age was 48 years old. The most common clinical symptoms were fever (187 patients; 63%) and cough (174 patients; 58.6%). The predominant descriptive chest imaging findings were ground-glass opacities and consolidation. Locations of abnormalities were bilateral, mainly distributed peripherally, in the lower lung zones, and in the middle lung zones.
CONCLUSIONS: This study provides an understanding of the most common clinical and radiological features of patients with laboratory-confirmed COVID-19 in Saudi Arabia. The majority of COVID-19 patients in our study cohort had either stable or worse progression of lung lesions during follow-ups; thus, they presented moderate disease cases. Elderly males were more affected by COVID-19 than females, with fever and cough being the most common clinical symptoms.
Keywords: COVID-19, multidetector computed tomography, Radiography, Adolescent, COVID-19, Female, Humans, Respiratory Tract Infections, SARS-CoV-2, Saudi Arabia, young adult
Background
Coronavirus disease 2019 (COVID-19) is a viral respiratory disease that first emerged in Wuhan, China, in December 2019. It quickly spread worldwide with increasing numbers of infected people and deaths [1,2]. Accordingly, the World Health Organization declared it a public health emergency of international concern on January 30, 2020 [3]. As of March 2, 2020, the Ministry of Health in Saudi Arabia confirmed the first case of COVID-19 in the kingdom [4,5]. By May 20, 2021, more than 437 569 cases, including 7214 deaths from COVID-19, had been recorded in Saudi Arabia [6]. Early diagnosis and detection are important to isolate suspected COVID-19 cases and control the outbreak [7].
The most common clinical symptoms of COVID-19 are fever, cough, and shortness of breath [8–10]. These symptoms may appear 3–6 days after exposure, based on the virus’s incubation period of 0–14 days being assumed by the World Health Organization [11]. The current criterion standard clinical diagnostic tool for COVID-19 is the reverse transcription polymerase chain reaction (RT-PCR) analysis extracted from a saliva or mucus swab sample [12]. However, there are a number of variables affecting their sensitivity in clinical practice, including the stage of infection, specimen type and handling, and the sufficiency of the specimen [13,14]. Thus, suspected COVID-19 cases need to be isolated during the RT-PCR test processing time to reduce the risk of disease transmission [13,14]. In addition, the main concern during a pandemic is about the availability of RT-PCR testing. Therefore, chest radiological examinations with CT and/or X-rays have been used in several studies along with RT-PCR for the early diagnosis and management of COVID-19 progression [7,9,12,15–20].
Recently, most of the published studies of chest imaging findings in patients with COVID-19 have been exclusively based in China and focused on CT manifestations [2,15,16,18,21–30]. To the best of our knowledge, information regarding imaging features of patients infected with COVID-19 in the Saudi Arabian population is scarce. In this study, we aimed to explore the chest imaging findings and clinical characteristics of patients with laboratory-confirmed COVID-19 admitted to government hospitals in Jeddah, Saudi Arabia.
Material and Methods
STUDY DESIGN AND PARTICIPANTS:
This was a retrospective, multi-center case series study that included 305 laboratory-confirmed COVID-19 cases. Data related to COVID-19 cases were collected from 4 government institutions (King Fahad General Hospital, King Abdullah Medical Complex, East Jeddah Hospital, and King Abdul-Aziz Hospital) in Jeddah, Saudi Arabia, from May 15 to July 10, 2020. Inclusion criteria were patients being at least 18 years old, having laboratory confirmation of COVID-19 infection via real-time RT-PCR, and having undergone a chest radiological examination. We excluded all suspected cases without evidence of laboratory confirmation of COVID-19 infection despite having symptoms or patients who had positive RT-PCR results but were discharged for home isolation without diagnosis via chest imaging.
DATA COLLECTION:
Information on patient demographics, signs and symptoms, co-morbid medical conditions, laboratory results, and radiological findings retrospectively extracted from patients’ paper and electronic medical records were collected by research coordinators and cross-checked by research investigators. All data were collected at the time of the patient’s admission. The patients’ medical record numbers were hidden from the data header to ensure the confidentially of all data.
Through laboratory investigation, amplification of the genetic material was extracted from the saliva or mucus swab sample through an RT-PCR. The final results were categorized as negative or positive in the study analysis. The date of disease onset was defined as the day when the first symptom was noticed.
The COVID-19 disease severity was classified into mild, moderate, and severe cases based on laboratory, clinical, and radiological findings. Laboratory-confirmed COVID-19 patients asymptomatic or with clinical symptoms and an absence of radiological findings of pneumonia were classified as mild cases. Moderate cases were defined as laboratory-confirmed COVID-19 patients with clinical symptoms and the presence of radiographic signs of pneumonia. Severe cases were defined as laboratory-confirmed COVID-19 patients with severe clinical symptoms or critically ill COVID-19 patients admitted to intensive care units (ICU) due to respiratory failure requiring invasive mechanical ventilation, organ failure, or shock and the presence of more severe radiographic signs such as pulmonary infiltration > 50% of the lung field.
RADIOLOGICAL ASSESSMENT:
Chest X-rays were acquired in the routine postero-anterior projection with full inspiration or in the antero-posterior projection in cases of supine patients using digital or portable chest X-ray machines. All laboratory-confirmed COVID-19 patients in our study cohort were initially screened with chest X-rays. CT scans were only performed for evaluation of progressed severe cases during follow-ups or for assessment of complications of COVID-19 pneumonia. CT imaging was performed using a multi-detector CT scanner with 64 channels with the following scanners: Somatom Emotion (Siemens Healthcare), HiSpeed-Dual (GE Healthcare), and 64-MDCT LightSpeed VCT (GE Healthcare). The acquisition parameters for CT examinations were as follows: tube voltage, 120 kVp; 100–150 mAs; collimation, 0.625–5 mm; pitch, 0.75–1.5; and image reconstruction (slice thickness, 1.25 mm/interval, 1.25 mm). All scans were done from the upper level of the thoracic inlet to the inferior level of costophrenic angle. CT examinations were conducted without a contrast medium with the patient in supine position at full inspiration. To further examine pulmonary embolism, CT pulmonary angiograms were performed with intravenous contrast administration.
All radiological examinations, including chest X-rays and CT scans or follow-up examinations performed for confirmed COVID-19 patients, were interpreted by consultant radiologists with more than 10 years of experience in chest imaging. Consultant radiologists were blinded to the subjects’ clinical outcomes. Then, the radiological images were determined to be normal or abnormal. A normal chest image was defined as being devoid of lung opacities and the absence of pleural effusion and pneumothorax. Chest images with opacities were considered abnormal and were assessed for predominate distribution of opacities and patterns.
Radiological images, including chest X-rays and CT scans, were evaluated for the presence of the following features: lung opacities that could be ground-glass opacities and/or consolidation, pleural effusion or pneumothorax, linear atelectasis, reticulation, distribution within the lung (peripheral, perihilar, central, or diffuse), laterality (right, left, or bilateral), involved lung field (upper, lower, or middle zones), and their progression on follow-up images (stable, worse, or improved). Other radiological features were also investigated, such as peribronchial wall thickening, pulmonary embolism, air bronchogram signs, interlobular septal thickening, subpleural, mediastinal lymphadenopathy, and pulmonary nodules.
ETHICAL CONSIDERATION:
This study was approved by the institutional review board at the Ministry of Health in Saudi Arabia, registration number KACST, KSA: H-02-J-002. Patients were informed that their personal information will be kept confidential and their clinical data and radiological images will be used for research purposes in this project. A written consent form was waived due to the retrospective, observational nature of the study.
STATISTICAL ANALYSIS:
Statistical analysis was performed using SPSS version 25.0 (IBM). Descriptive statistical analysis was used to describe patients’ demographics, clinical characteristics, radiological findings, and laboratory findings. The independent samples
Results
DEMOGRAPHIC AND CLINICAL CHARACTERISTICS:
The original study cohort of COVID-19 cases included 311 participants. Of these participants, a total of 297 who had laboratory-confirmed COVID-19 patients and who underwent chest imaging were included in our study analysis. Demographic and clinical characteristics of all patients included in the present study are summarized in Table 1. The mean (± standard deviation) age of patients was 48 (±14.3) years. The majority of patients who had positive RT-PCR results were in the age range of 46–55 (Table 1). In addition, moderate cases were more prevalent in this age group (61%) (Figure 1), and among males (n=155) more than females (n=32) (Figure 2).
RADIOLOGICAL FINDINGS:
Tables 2 and 3 provide the chest imaging finding of laboratory-confirmed COVID-19 patients. The majority of COVID-19 patients had abnormal radiological findings, bilateral in nature, of which ground-glass opacities and consolidations were most frequent, mainly involved within the lower and middle lung zones. The predominate chest X-ray findings is shown in Figure 3.
The pulmonary involvement of lung lesions on chest CT images of COVID-19 patients most commonly found in multiple lung zones (middle and lower lung zones), bilaterally and peripherally distributed (Table 3). Seven patients (33.3%) presented with diffuse scattered patchy ground-glass opacities and/or consolidations within the lung. None of our participants had only central distribution and 4 patients had no axial lung distribution on CT images (Table 3). Figures 4A, 4B and 5A–5C show the predominate chest CT imaging features of laboratory-confirmed COVID-19 patients.
Other imaging features found on chest CT images of COVID-19 patients were air bronchogram signs (52.4%), atelectasis (42.9%), and subpleural lines (33.3%). Pleural effusion, pneumothorax, pulmonary nodules, and pulmonary embolism were found in a small number of patients (Table 3). Mediastinal lymphadenopathy was less common in COVID-19 patients.
Discussion
The present study found that most patients with laboratory-confirmed COVID-19 had typical imaging features, including ground-glass opacity lesions and consolidation, that are peripherally distributed, bilaterally involved, and predominantly in the lower and middle lung zones. In addition, the majority of COVID-19 patients in our study cohort had either stable or worse progression of lung lesions during follow-ups; thus, they presented moderate disease cases. The most common clinical symptoms were fever and cough. The mean age group infected with COVID-19 was 41–60 years, and males were affected more than females.
Chest imaging plays an important role in the diagnosis of COVID-19 [7,17,31]. Radiological features such as ground-glass opacity and consolidation that were present in our study cohort are similar to those of the imaging features of COVID-19 presented in previously published studies in China and other countries [15,18,19,26,29,32–37]. These are the hallmarks of COVID-19 in chest X-rays and CT imaging [18,29,32,37,38]. Regarding lesion distribution, patients with laboratory-confirmed COVID-19 in the present study were more likely to have peripheral distribution, bilateral involvement, and lower and middle lung predominance in chest imaging, which is consistent with results of previous studies [15,34,37–39].
The chest X-ray is considered a routine imaging modality for diagnosis and monitoring the care of patients with COVID-19 [17]. It helps in evaluating lung abnormalities for screening out patients with positive RT-PCR screening results [15,29]. Despite chest CT scans having high sensitivity for the early identification of lung lesions and diagnosis of patients with COVID-19 [19,21,40], only a few patients in our study cohort had chest CT examinations. Most of these patients were initially screened with chest X-rays and then had CT scans when they progressed to severe cases during follow-ups. According to the American College of Radiology, CT scans are not recommended for use as a first-line test for the diagnosis of COVID-19 [41]. Therefore, CT scans can only be performed after the detection of abnormalities in chest X-rays of laboratory-confirmed COVID-19 patients or after screening patients with COVID-19 pneumonia complications [17,42,43]. Portable chest X-ray units are usually used for patients with COVID-19 to reduce infection risks in radiology departments [29].
Fever, cough, and dyspnea were the most common clinical symptoms in COVID-19 patients in our cohort. These clinical symptoms are in line with findings from a recent study by Saleemi et al [44] in Riyadh, Saudi Arabia. Their study found that 59% of their COVID-19 patients had mild COVID-19, whereas 41% were categorized as severe cases [44]. Compared with that study, our study consisted of a larger number of hospitalized COVID-19 patients from different government hospitals in Jeddah, Saudi Arabia. In addition, we categorized the patients as mild, moderate, and severe COVID-19 cases. We found that the majority of laboratory-confirmed COVID-19 patients (63%) were moderate cases, whereas only 27.6% were mild and 9.4% were severe cases. Notably, 39 cases (13.1%) of confirmed positive COVID-19 in our study cohort were asymptomatic. This result suggests that laboratory tests and/or chest imaging should be done for asymptomatic individuals who are at high risk due to a history of contact with positive or suspected COVID-19 patients for early detection of the disease [34,42,45].
In the present study, we observed a greater number of males infected with COVID-19 than females, and most of the male cases were moderate. This finding is in agreement with previously published studies [9,46]. More males have also been found to be infected with the Middle East respiratory syndrome coronavirus (MERS-CoV) and severe acute respiratory syndrome coronavirus infection (SARS-CoV) than females [47,48]. The protection of steroid hormones and factors related to sex chromosomes play an important role in innate and adaptive immunity, which reduces the susceptibility of females to viral infection [49–51]. Additionally, recent evidence revealed that high-risk lifestyle behaviors and preexisting comorbidities may also play a role in increased mortality and responses to COVID-19 among elderly men [52–54].
The main strength of our study is that it included a large number of participants with laboratory-confirmed COVID-19 from different government hospitals in Jeddah, Saudi Arabia. In addition, the study explored all the different radiological features from both chest X-rays and CT images. However, the study had some limitations. First, it included only positive laboratory-confirmed COVID-19 cases; negative results or suspected cases were not included in the analysis. Comprehensive investigation of the imaging features of suspected COVID-19 patients with negative results and confirmed positive results to differentiate COVID-19 pneumonia from other lung-infection diseases is recommended. Second, we did not have follow-up CT images in our cohort to explore changes in CT imaging features and compare them with clinical parameters for patients with severe cases. This could help in the management of disease progression and outcome prediction to support clinical decision making [39]. Further research is needed to evaluate the relationship between chest imaging features and clinical characteristics in COVID-19 cases in Saudi Arabia.
Conclusions
This study describes the radiology and clinical features of patients with confirmed COVID-19 in Saudi Arabia. The imaging pattern of laboratory-confirmed COVID-19 patients was bilateral peripheral ground-glass opacities and consolidation involving the lower and middle lung zones. Elderly males were more affected by COVID-19 than females, with fever and cough being the most common clinical symptoms. The present study demonstrates clinical and radiological characteristics of COVID-19 similar to previous studies reported worldwide. Our study suggests that combining evaluation of radiological features with laboratory and clinical findings could help in early diagnosis of COVID-19.
Figures
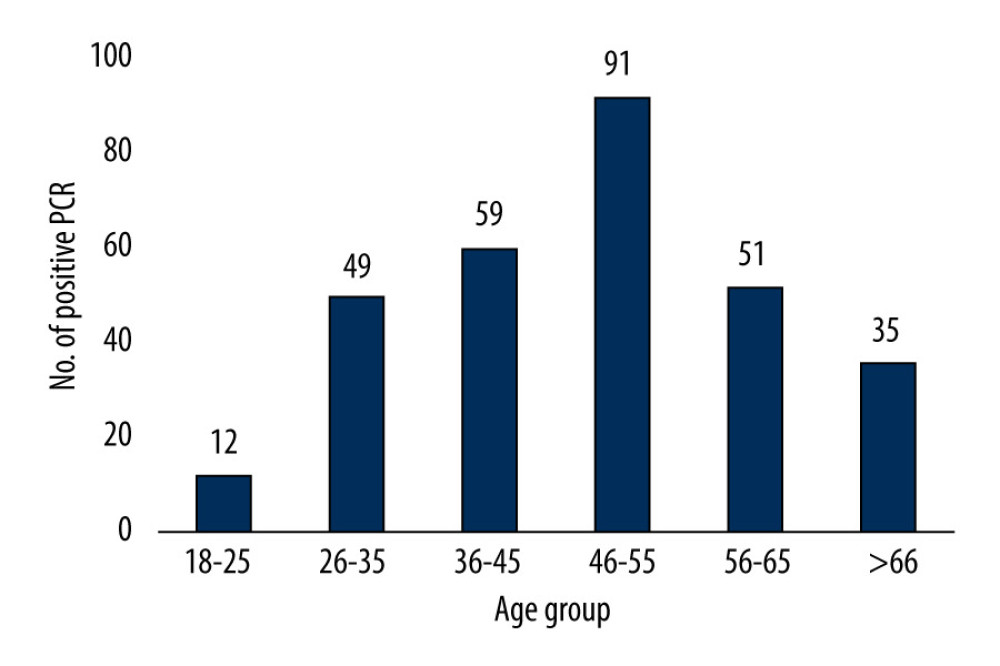 Figure 1. Disease severity stratified by age.
Figure 1. Disease severity stratified by age. 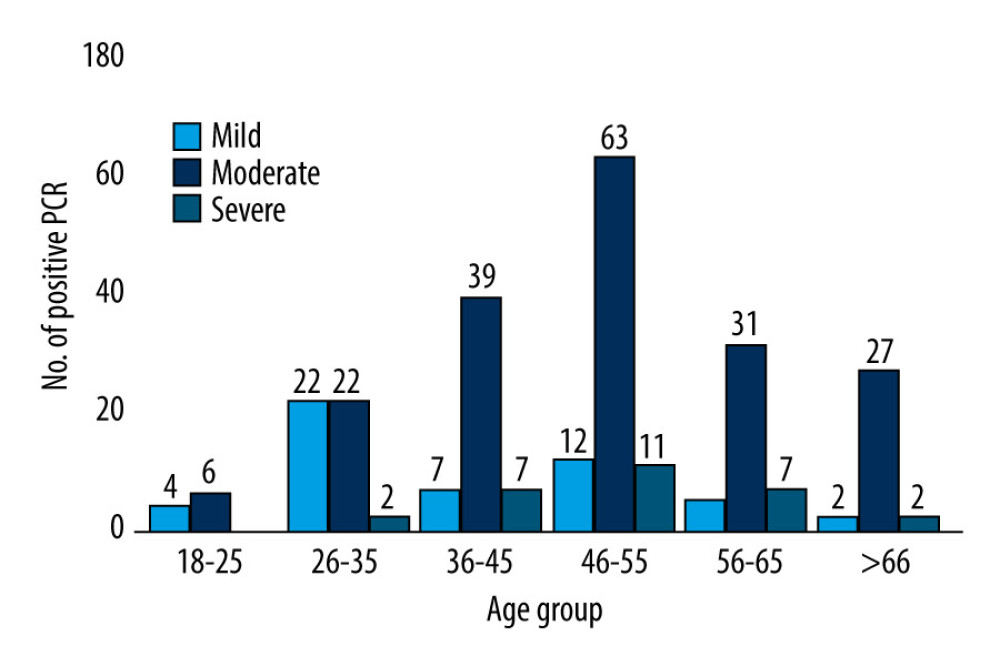 Figure 2. Disease severity stratified by sex.
Figure 2. Disease severity stratified by sex. 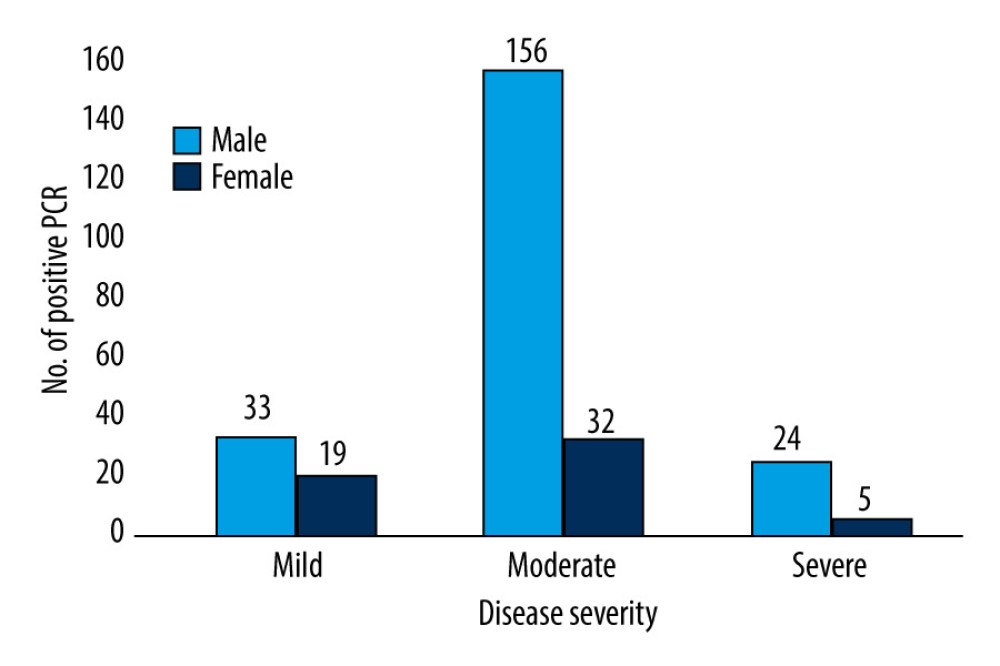 Figure 3. Chest X-ray of a patient with laboratory-confirmed COVID-19 shows bilateral patchy ground-glass opacities (digital portable X-ray machine: Siemens mobilett mira).
Figure 3. Chest X-ray of a patient with laboratory-confirmed COVID-19 shows bilateral patchy ground-glass opacities (digital portable X-ray machine: Siemens mobilett mira). 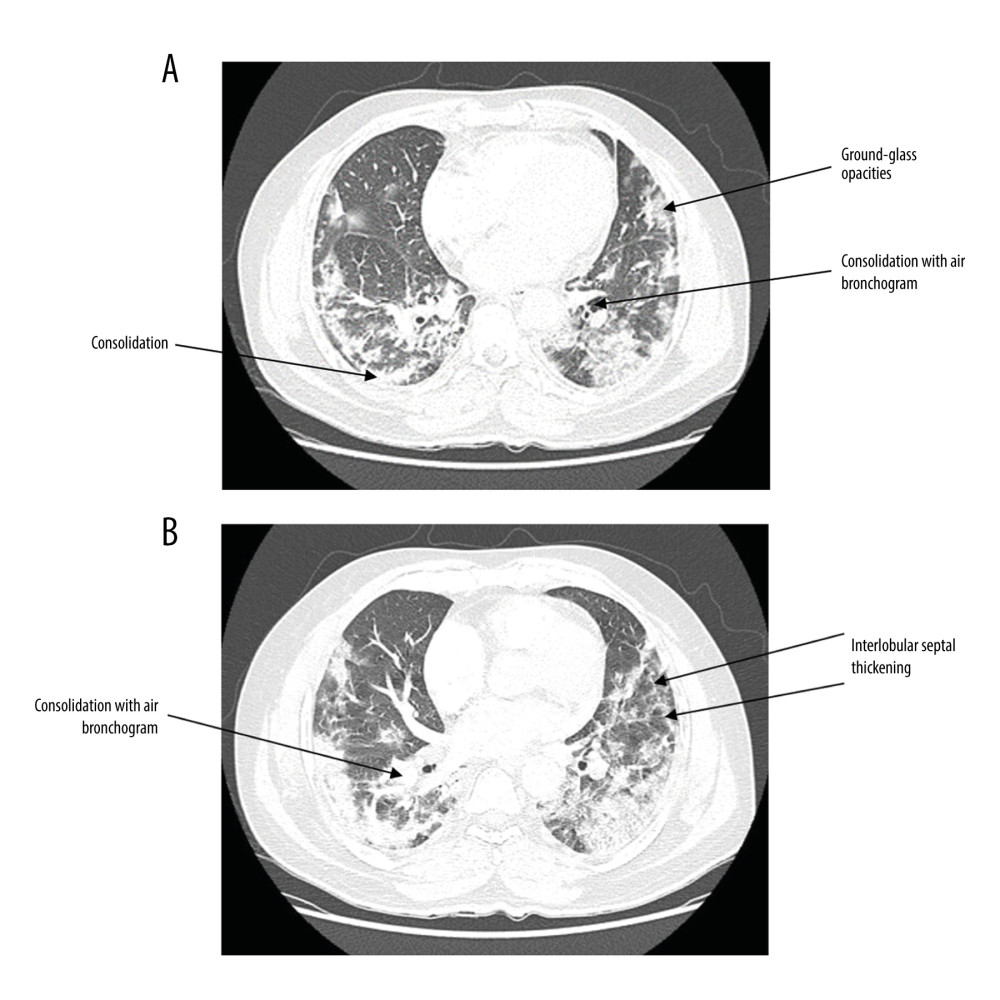 Figure 4. (A) CT scan of patient with laboratory-confirmed COVID-19 shows bilateral scattered areas of peripheral consolidation and ground-glass opacities (CT scan: GE discovery CT750 hd). (B) CT scan of patient with laboratory-confirmed COVID-19 shows minimal interlobular septal thickening and right upper perihilar consolidation with air bronchogram (CT scan: GE discovery CT750 hd).
Figure 4. (A) CT scan of patient with laboratory-confirmed COVID-19 shows bilateral scattered areas of peripheral consolidation and ground-glass opacities (CT scan: GE discovery CT750 hd). (B) CT scan of patient with laboratory-confirmed COVID-19 shows minimal interlobular septal thickening and right upper perihilar consolidation with air bronchogram (CT scan: GE discovery CT750 hd). 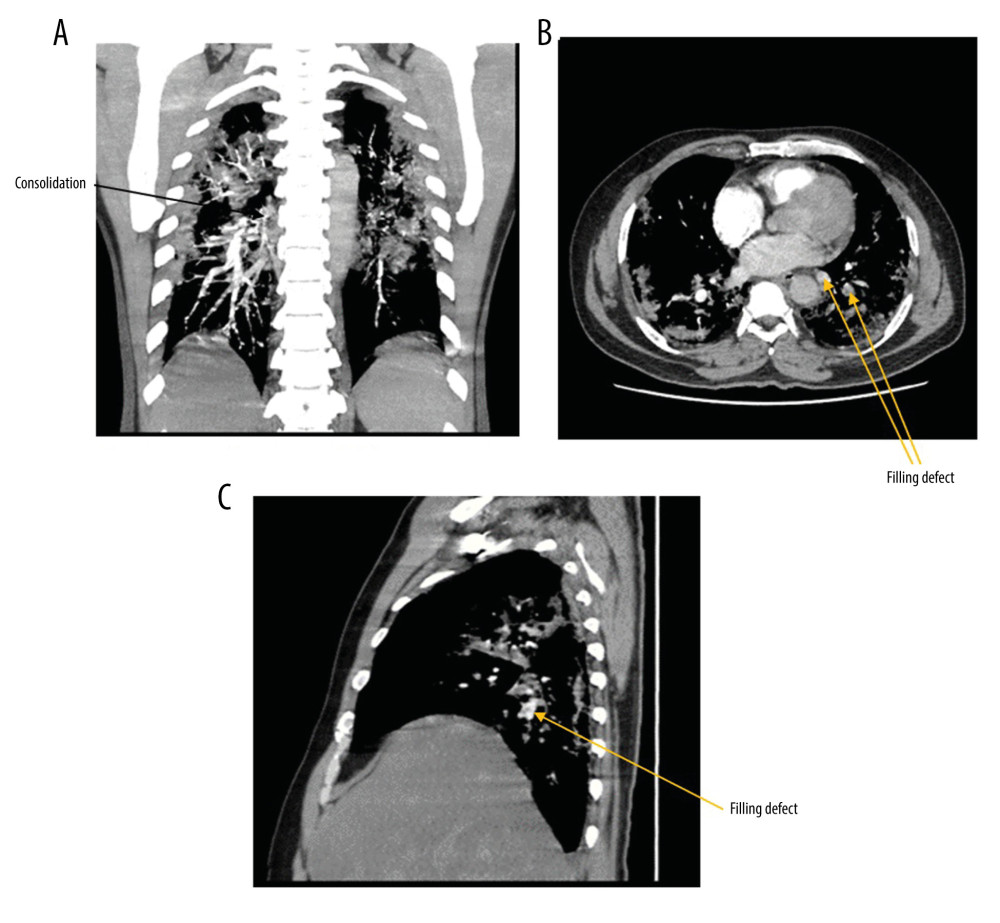 Figure 5. (A) CT pulmonary angiogram with intravenous contrast administration of a patient with COVID-19 shows bilateral scattered areas of peripheral consolidation, and ground-glass opacities (CT scan: GE discovery CT750 hd). (B) CT pulmonary angiogram with intravenous contrast administration of a patient with COVID-19 shows a filling defect noted in the left lower lobar artery (CT scan: GE discovery CT750 hd). (C) CT pulmonary angiogram with intravenous contrast administration of a patient with COVID-19 shows a filling defect extending to the segmental branches (CT scan: GE discovery CT750 hd).
Figure 5. (A) CT pulmonary angiogram with intravenous contrast administration of a patient with COVID-19 shows bilateral scattered areas of peripheral consolidation, and ground-glass opacities (CT scan: GE discovery CT750 hd). (B) CT pulmonary angiogram with intravenous contrast administration of a patient with COVID-19 shows a filling defect noted in the left lower lobar artery (CT scan: GE discovery CT750 hd). (C) CT pulmonary angiogram with intravenous contrast administration of a patient with COVID-19 shows a filling defect extending to the segmental branches (CT scan: GE discovery CT750 hd). References
1. Kanne JP, Chest CT findings in 2019 novel coronavirus (2019-nCoV) infections from Wuhan, China: Key points for the radiologist: Radiology, 2020; 295(1); 16-17
2. Zhou S, Wang Y, Zhu T, Xia L, CT features of coronavirus disease 2019 (COVID-19) pneumonia in 62 patients in Wuhan, China: Am J Roentgenol, 2020; 214(6); 1287-94
3. Sohrabi C, Alsafi Z, O’Neill N, World Health Organization declares global emergency: A review of the 2019 novel coronavirus (COVID-19): Int J Surg, 2020; 76; 71-76 [Erratum in: Int J Surg. 2020 May;77: 217]
4. Barry M, Ghonem L, Alsharidi A, Coronavirus disease-2019 pandemic in the Kingdom of Saudi Arabia: Mitigation measures and hospital preparedness: Journal of Nature and Science of Medicine, 2020; 3(3); 155
5. Barry M, Al Amri M, Memish ZA, COVID-19 in the Shadows of MERS-CoV in the Kingdom of Saudi Arabia: J Epidemiol Glob Health, 2020; 10(1); 1-3
6. Ministry of health in Saudi Arabia [in Arabian]https://covid19.moh.gov.sa
7. Yang W, Sirajuddin A, Zhang X, The role of imaging in 2019 novel coronavirus pneumonia (COVID-19): Eur Radiol, 2020; 30(9); 4874-82
8. Zhang G, Zhang J, Wang B, Analysis of clinical characteristics and laboratory findings of 95 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A retrospective analysis: Respir Res, 2020; 21(1); 74
9. Chen N, Zhou M, Dong X, Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study: Lancet (London, England), 2020; 395(10223); 507-13
10. Huang C, Wang Y, Li X, Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China: Lancet (London, England), 2020; 395(10223); 497-506
11. Backer JA, Klinkenberg D, Wallinga J, Incubation period of 2019 novel coronavirus (2019-nCoV) infections among travellers from Wuhan, China, 20–28 January 2020: Eurosurveillance, 2020; 25(5); 2000062
12. Long C, Xu H, Shen Q, Diagnosis of the coronavirus disease (COVID-19) : rRT-PCR or CT?: Eur J Radiol, 2020; 126; 108961
13. Li Y, Yao L, Li J, Stability issues of RT-PCR testing of SARS-CoV-2 for hospitalized patients clinically diagnosed with COVID-19: J Med Virol, 2020; 92(7); 903-8
14. Ai T, Yang Z, Hou H, Correlation of chest CT and RT-PCR testing in coronavirus disease 2019 (COVID-19) in China: A report of 1014 cases: Radiology, 2020; 296(2); E32-40
15. Wong HYF, Lam HYS, Fong AH-T, Frequency and distribution of chest radiographic findings in COVID-19 positive patients: Radiology, 2020; 296(2); E72-78
16. Wang K, Kang S, Tian R, Imaging manifestations and diagnostic value of chest CT of coronavirus disease 2019 (COVID-19) in the Xiaogan area: Clin Radiol, 2020; 75(5); 341-47
17. Rubin GD, Ryerson CJ, Haramati LB, The role of chest imaging in patient management during the COVID-19 pandemic: A multinational consensus statement from the fleischner society: Chest, 2020; 158(1); 106-16
18. Kong W, Agarwal PP, Chest imaging appearance of COVID-19 infection: Radiol Cardiothorac Imaging, 2020; 2(1); e200028
19. Ng M-Y, Lee EY, Yang J, Imaging profile of the COVID-19 infection: Radiologic findings and literature review: Radiol Cardiothorac Imaging, 2020; 2(1); e200034
20. Shahzeb M, Khan A, Muhammad A, Detection of coronavirus disease (COVID-19) using radiological examinations: J Pure Appl Microbiol, 2020; 14; 911-20 20200429
21. Pan Y, Guan H, Zhou S, Initial CT findings and temporal changes in patients with the novel coronavirus pneumonia (2019-nCoV): A study of 63 patients in Wuhan, China: Eur Radiol, 2020; 30(6); 3306-9
22. Xu YH, Dong JH, An WM, Clinical and computed tomographic imaging features of novel coronavirus pneumonia caused by SARS-CoV-2: J Infect, 2020; 80(4); 394-400
23. Yang W, Cao Q, Qin L, Clinical characteristics and imaging manifestations of the 2019 novel coronavirus disease (COVID-19): A multi-center study in Wenzhou city, Zhejiang, China: J Infect, 2020; 80(4); 388-93
24. Zhao W, Zhong Z, Xie X, Yu Q, Liu J, CT scans of patients with 2019 novel coronavirus (COVID-19) pneumonia: Theranostics, 2020; 10(10); 4606
25. Zhong Q, Li Z, Shen XCT imaging features of patients with different clinical types of coronavirus disease 2019 (COVID-19): Zhejiang Da Xue Xue Bao Yi Xue Ban, 2020; 49(1); 198-202 [in Chinese]
26. Chung M, Bernheim A, Mei X, CT imaging features of 2019 novel coronavirus (2019-nCoV): Radiology, 2020; 295(1); 202-7
27. Salehi S, Abedi A, Balakrishnan S, Gholamrezanezhad A, Coronavirus disease 2019 (COVID-19): A systematic review of imaging findings in 919 patients: Am J Roentgenol, 2020; 215; 87-93
28. Li X, Zeng W, Li X, CT imaging changes of corona virus disease 2019(COVID-19): A multi-center study in Southwest China: J Transl Med, 2020; 18(1); 154
29. Jacobi A, Chung M, Bernheim A, Eber C, Portable chest X-ray in coronavirus disease-19 (COVID-19): A pictorial review: Clin Imaging, 2020; 64; 35-42
30. Lomoro P, Verde F, Zerboni F, COVID-19 pneumonia manifestations at the admission on chest ultrasound, radiographs, and CT: Single-center study and comprehensive radiologic literature review: Eur J Radiol Open, 2020; 7; 100231
31. Dong D, Tang Z, Wang S, The role of imaging in the detection and management of COVID-19: A review: IEEE Rev Biomed Eng, 2021; 14; 16-29
32. He X, Zheng J, Ren J, Zheng G, Liu L, Chest high-resolution computed tomography imaging findings of coronavirus disease 2019 (COVID-19) pneumonia: International Journal of Radiation Research, 2020; 18(2); 343-49
33. Li X, Zeng W, Li X, CT imaging changes of corona virus disease 2019 (COVID-19): A multi-center study in Southwest China: J Transl Med, 2020; 18(1); 154
34. Shi H, Han X, Jiang N, Radiological findings from 81 patients with COVID-19 pneumonia in Wuhan, China: A descriptive study: Lancet Infect Dis, 2020; 20(4); 425-34
35. Yoon SH, Lee KH, Kim JY, Chest radiographic and CT findings of the 2019 novel coronavirus disease (COVID-19): Analysis of nine patients treated in Korea: Korean J Radiol, 2020; 21(4); 494-500
36. Zhou Z, Guo D, Li C, Coronavirus disease 2019: Initial chest CT findings: Eur Radiol, 2020; 30(8); 4398-406
37. Wu J, Wu X, Zeng W, Chest CT findings in patients with coronavirus disease 2019 and its relationship with clinical features: Invest Radiol, 2020; 55(5); 257-61
38. Xu X, Yu C, Qu J, Imaging and clinical features of patients with 2019 novel coronavirus SARS-CoV-2: Eur J Nucl Med Mol Imaging, 2020; 47(5); 1275-80
39. Zhao W, Zhong Z, Xie X, Relation between chest CT findings and clinical conditions of coronavirus disease (COVID-19) pneumonia: A multicenter study: Am J Roentgenol, 2020; 214(5); 1072-77
40. Li B, Li X, Wang Y, Han Y, Diagnostic value and key features of computed tomography in coronavirus disease 2019: Emerg Microbes Infect, 2020; 9(1); 787-93
41. Radiology ACo, ACR recommendations for the use of chest radiography and computed tomography (CT) for suspected COVID-19 infection: ACR website, 2020
42. Shirani K, Sheikhbahaei E, Torkpour Z, A narrative review of COVID-19: the new pandemic disease: Iran J Med Sci, 2020; 45(4); 233-49
43. Raptis CA, Hammer MM, Short RG, Chest CT and coronavirus disease (COVID-19): A critical review of the literature to date: Am J Roentgenol, 2020; 215(4); 839-42
44. Saleemi S, Alhajji M, Almaghrabi R, Clinical characteristics of patients with COVID-19 in Saudi Arabia-a single center experience: Res Rev Infect Dis, 2020; 3(1); 68-74
45. Feng Z, Yu Q, Yao S, Early prediction of disease progression in COVID-19 pneumonia patients with chest CT and clinical characteristics: Nat Commun, 2020; 11(1); 1-9
46. Wang D, Hu B, Hu C, Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus – infected pneumonia in Wuhan, China: JAMA, 2020; 323(11); 1061-69
47. Badawi A, Ryoo SG, Prevalence of comorbidities in the Middle East respiratory syndrome coronavirus (MERS-CoV): A systematic review and meta-analysis: Int J Infect Dis, 2016; 49; 129-33
48. Channappanavar R, Fett C, Mack M, Sex-based differences in susceptibility to severe acute respiratory syndrome coronavirus infection: J Immunol, 2017; 198(10); 4046-53
49. Jaillon S, Berthenet K, Garlanda C, Sexual dimorphism in innate immunity: Clin Rev Allergy Immunol, 2019; 56(3); 308-21
50. Conti P, Younes A, Coronavirus COV-19/SARS-CoV-2 affects women less than men: Clinical response to viral infection: J Biol Regul Homeost Agents, 2020; 34(2); 393-43
51. Papadopoulos V, Li L, Samplaski M, Why does COVID-19 kill more elderly men than women? Is there a role for testosterone?: Andrology, 2021; 9(1); 65-72
52. Griffith DM, Sharma G, Holliday CS, Men and COVID-19: a biopsychosocial approach to understanding sex differences in mortality and recommendations for practice and policy interventions: Prev Chronic Dis, 2020; 17; E63
53. Haitao T, Vermunt J, Abeykoon J, COVID-19 and sex differences: Mechanisms and biomarkers: Elsevier, Mayo Clinic Proceedings, 2020
54. Agrawal H, Das N, Nathani S, An assessment on impact of COVID-19 infection in a gender specific manner: Stem Cell Rev Rep, 2021; 17(1); 94-112
Figures
Figure 1. Disease severity stratified by age.Figure 2. Disease severity stratified by sex.Figure 3. Chest X-ray of a patient with laboratory-confirmed COVID-19 shows bilateral patchy ground-glass opacities (digital portable X-ray machine: Siemens mobilett mira).Figure 4. (A) CT scan of patient with laboratory-confirmed COVID-19 shows bilateral scattered areas of peripheral consolidation and ground-glass opacities (CT scan: GE discovery CT750 hd). (B) CT scan of patient with laboratory-confirmed COVID-19 shows minimal interlobular septal thickening and right upper perihilar consolidation with air bronchogram (CT scan: GE discovery CT750 hd).Figure 5. (A) CT pulmonary angiogram with intravenous contrast administration of a patient with COVID-19 shows bilateral scattered areas of peripheral consolidation, and ground-glass opacities (CT scan: GE discovery CT750 hd). (B) CT pulmonary angiogram with intravenous contrast administration of a patient with COVID-19 shows a filling defect noted in the left lower lobar artery (CT scan: GE discovery CT750 hd). (C) CT pulmonary angiogram with intravenous contrast administration of a patient with COVID-19 shows a filling defect extending to the segmental branches (CT scan: GE discovery CT750 hd). Tables
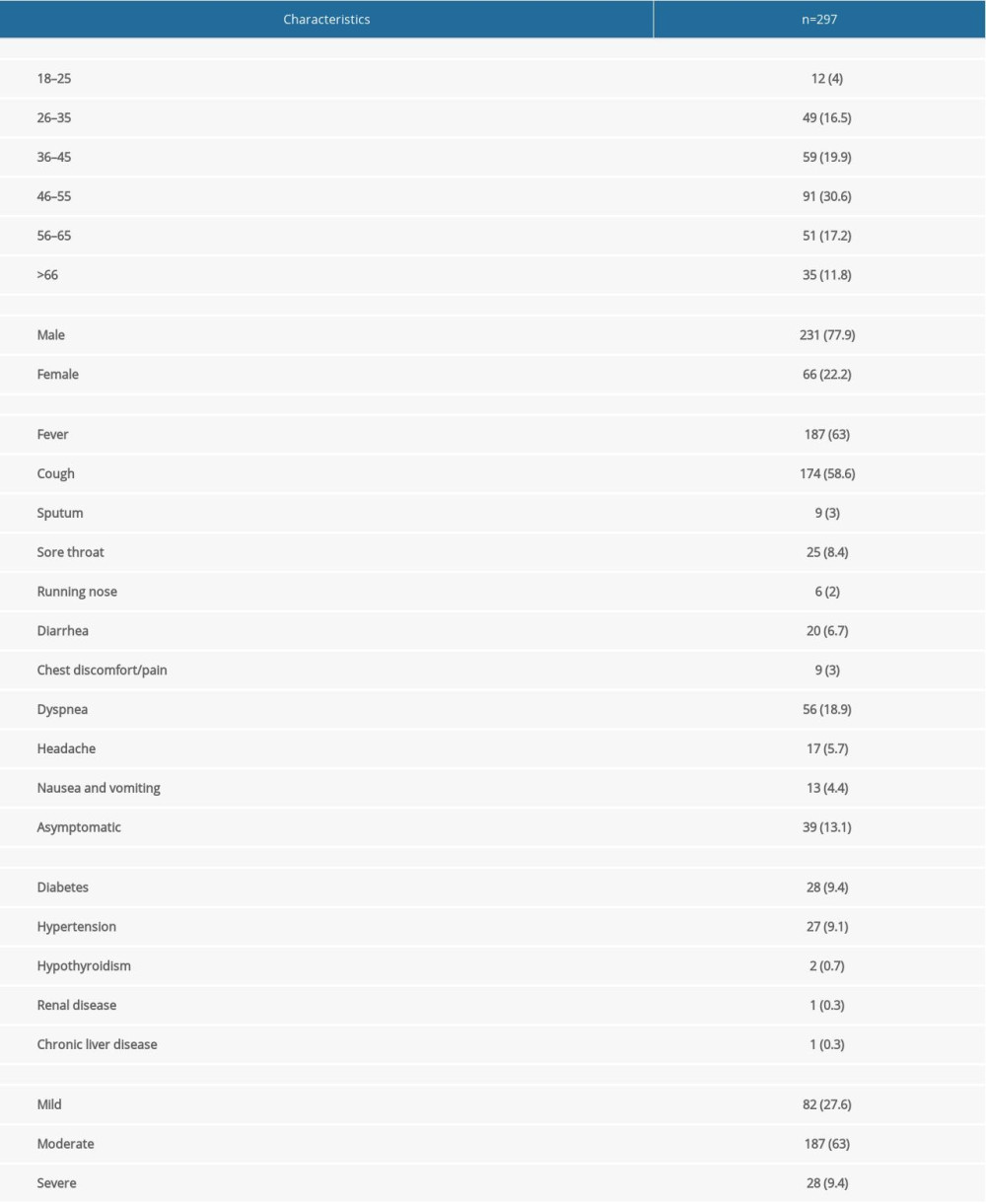 Table 1. Demographic and clinical characteristics of patients with COVID-19.
Table 1. Demographic and clinical characteristics of patients with COVID-19.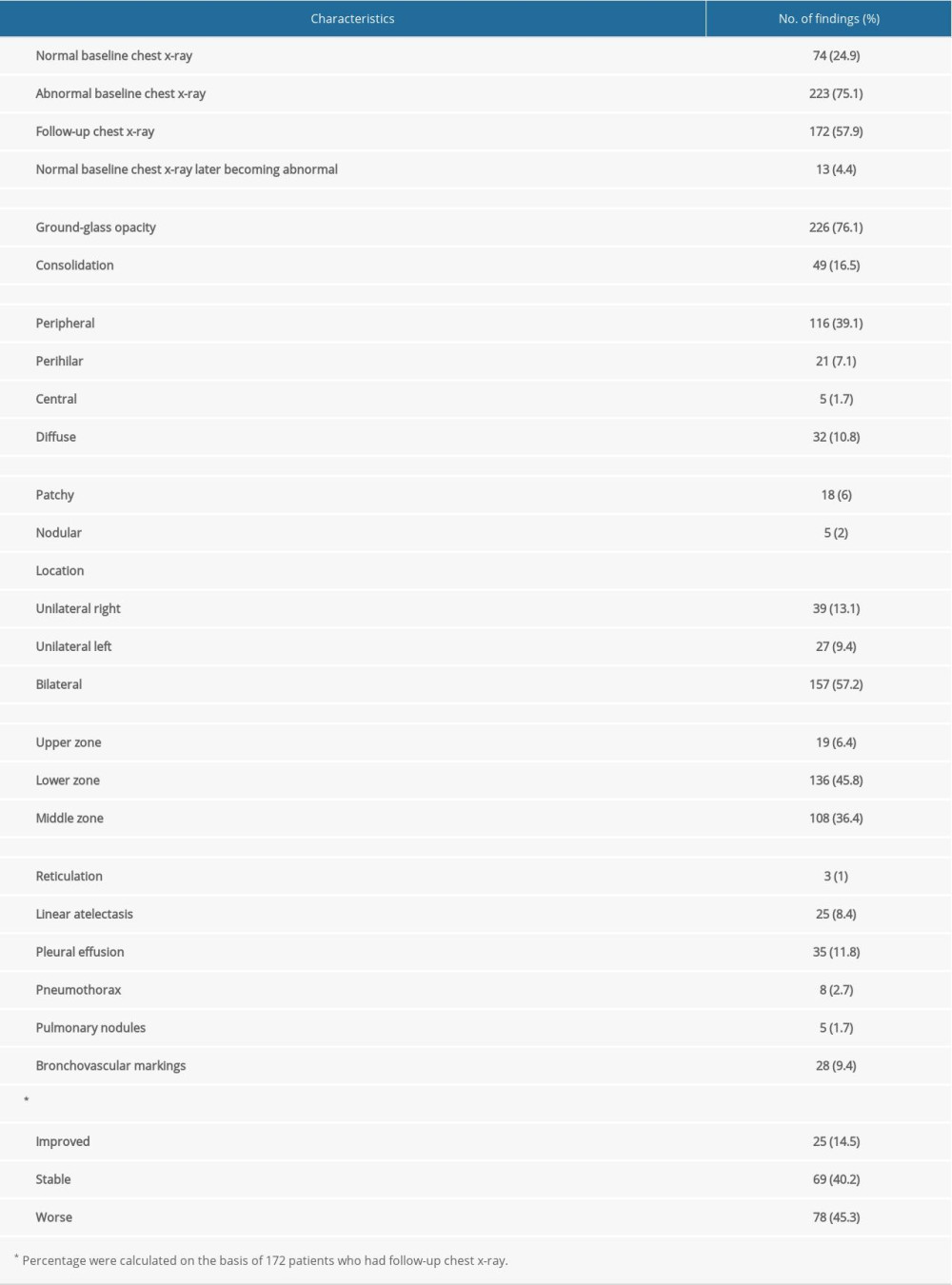 Table 2. Radiological findings on chest X-rays (n=297).
Table 2. Radiological findings on chest X-rays (n=297).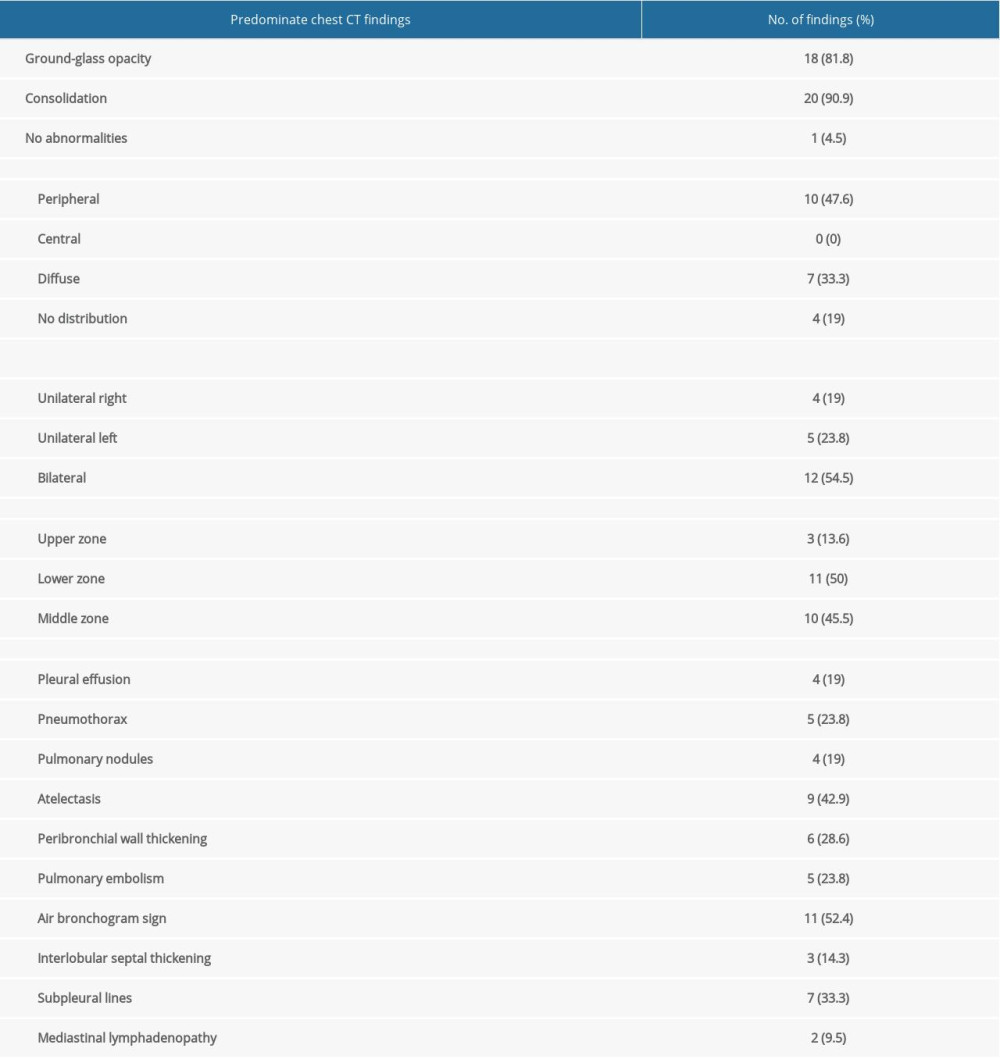 Table 3. Chest CT findings (n=22).Table 1. Demographic and clinical characteristics of patients with COVID-19.Table 2. Radiological findings on chest X-rays (n=297).Table 3. Chest CT findings (n=22).
Table 3. Chest CT findings (n=22).Table 1. Demographic and clinical characteristics of patients with COVID-19.Table 2. Radiological findings on chest X-rays (n=297).Table 3. Chest CT findings (n=22). In Press
Clinical Research
Institutional and Regional Variations in Access to Clinical Trials and Next-Generation Sequencing in Turkis...Med Sci Monit In Press; DOI: 10.12659/MSM.951027
Clinical Research
Low-Intensity Blood Flow-Restricted Multi-Joint Exercise Improves Muscle Function in Patients With Patellof...Med Sci Monit In Press; DOI: 10.12659/MSM.950516
Review article
Musculoskeletal Ultrasound and MRI in the Evaluation of Chemotherapy-Induced Peripheral Neuropathy: A ReviewMed Sci Monit In Press; DOI: 10.12659/MSM.951283
Clinical Research
Sensory Processing, Dissociation, and Affective Symptoms in Misophonia: A Cross-Sectional Study of 35 AdultsMed Sci Monit In Press; DOI: 10.12659/MSM.950938
Most Viewed Current Articles
17 Jan 2024 : Review article 10,187,196
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,708,487
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,341,643
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 706,524
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387