28 June 2021: Clinical Research
Factors Influencing Nurses’ Work Interruption in Wuhan Isolation Wards During the COVID-19 Pandemic
Xiao-Juan Zhou1AEF, Yuan-Yuan Dang2BC, Xia Wang3BC, Wen-Zhang Yang1CD, Wei Lu1DF, Jian-Hua Zhang1EF*DOI: 10.12659/MSM.929851
Med Sci Monit 2021; 27:e929851






Abstract
BACKGROUND: Through January 2021, the novel coronavirus (COVID-19) continued to create significant pressure on medical staff who have worked to treat patients with the disease and control its spread. This study aimed to increase understanding of the situation and influencing factors of nurses’ work interruption in Wuhan’s isolation ward during the COVID-19 pandemic.
MATERIAL AND METHODS: A self-designed general situation questionnaire and work interruption questionnaire were used to survey 160 nurses from Beijing, Chongqing, and Jilin who worked during the COVID-19 pandemic in Wuhan in March 2020. The questionnaire could only be answered once by each nurse via a WeChat account. The submitted answers were verified by 2 researchers.
RESULTS: The results showed that the rate of interruption of work among nurses in the isolation ward was 25%, and the rate of nurses experiencing a negative experience was 96.9%. The results of univariate analysis showed that the following factors were related to the work interruption of the nurses in the isolation ward (all P<0.05): emergency public incident training; emergency public incident treatment experience; knowledge of COVID-19 pneumonia; hours worked per shift in the quarantine area; and negative physiologic experience. Logistic regression analysis showed that negative experience, hours worked per shift, and emergency public incident training were the independent factors influencing work interruption among nurses in the isolation wards.
CONCLUSIONS: The incidence of interruption of work among nurses in the isolation ward was 25%. Negative experiences, long working hours per shift, and lack of emergency public incident training made the nurses more prone to work interruption.
Keywords: COVID-19, Hospitals, Isolation, Nurse Practitioners, Beijing, COVID-19, Emergency Service, Hospital, Nurses, Pandemics, Risk Factors, SARS-CoV-2, Surveys and Questionnaires, Workload
Background
Novel coronavirus (COVID-19) is a disease with a high rate of human-to-human transmission [1,2]. During the COVID-19 outbreak from January 2020 to April 2020 in Wuhan, medical staff from all over China went there to participate in the rescue work, becoming the core force of the rescue team (data come from National Health Commission of PRC: http://www.nhc.gov.cn/xcs/zhengcwj/202004/b90eb78d1dce4c6fab9bc58055cc6e96.shtml). Through April 16, 2020, a total of 68 128 COVID-19 cases were confirmed, with 4512 deaths, while 63 487 patients with COVID-19 were discharged (http://www.nhc.gov.cn/yjb/s7860/202004/6f8eb06d959f4ab7b56fe03236920be1.shtml). The medical staff, including nurses, played a significant role in responding to the emergency of the COVID-19 pandemic in Wuhan.
Through January 2021, a total of 102 083 344 COVID-19 cases were confirmed and 2 209 195 deaths occurred in 223 countries and regions, according to the data dashboard of the World Health Organization (https://www.who.int/emergencies/diseases/novel-coronavirus-2019). The rapid spread of COVID-19 had a negative impact on the population worldwide [3]. Throughout the COVID-19 pandemic of 2020, nurses made nursing history by aiding the high number of patients and working to prevent the spread of the disease [4]. The nurses required moral courage and resilience to work through the pandemic [4]. However, nursing work interruptions frequently occur in the intensive care unit and can harm patients [5]. When work periods are longer, more interruptions occur [6]. The COVID-19 isolation units are emergency care units, which require nurses to work for longer periods at high intensity, giving them increased work pressure. Therefore, nursing interruptions are expected in this type of environment.
Work interruptions refer to the cessation of work for various reasons within a prescribed time, role, and environment [7,8]. Study of the nursing interruptions among clinical frontline nurses during the COVID-19 pandemic and analysis of their influencing factors may provide a reference for the development of management countermeasures to reduce work interruptions in isolation wards. The aim of our study was to analyze the situation and the influencing factors of nurses’ work interruption in Wuhan’s isolation wards during the COVID-19 epidemic, providing reference for nurses’ emergency work in the future.
Material and Methods
PARTICIPANTS:
We had 4 medical workers as contacts in 4 hospitals, and each contact person established a WeChat group. They contacted the nurses from hospitals in Beijing, Chongqing, Wuhan, and Jilin via WeChat. The participants were chosen using convenience sampling. The questionnaire was sent to and collected from the participants via WeChat for the investigation. The nurses who volunteered to participate in this study must have worked in Wuhan during the COVID-19 pandemic. They were also required to report their real names, titles, and institutions and to identify the Wuhan isolation ward they worked in. Our medical workers in each group verified participant information and confirmed their participation. The inclusion criteria were as follows: The nurses must have worked as frontline clinical nurses in Wuhan during the COVID-19 epidemic; worked in a Wuhan isolation ward; and participated in epidemic prevention and control work for ≥7 days. All participants signed an informed consent form to volunteer their participation in the study.
DATA COLLECTION TOOLS:
This study used 2 data collection tools.
First, a nurse information form was designed by the researchers to collect the following: sex, age, marital status, job title, educational background, length of service, former department and affiliation (eg, intensive care unit, emergency department). It also asked the following: whether the nurse had participated in emergency public incident training; whether they had participated in emergency public incidents; whether they had prior experience participating in emergency public incidents; degree of knowledge about the prevention and control of SARS-CoV-2 infections; time worked in an isolation ward since the beginning of the pandemic; name of isolation ward where they worked in Wuhan; and the length of each shift. The form was designed according to published research on nurses’ protective exposure risk events during the COVID-19 pandemic [9].
Second, a work interruption survey was designed based on the published research on interruptions in healthcare [10]. Six experts were consulted, including 1 infection control expert, 1 nursing manager, and 4 clinical nurses, 3 of which were involved in the frontline work of the SARS epidemic in 2003. The following criteria were used to select the experts: more than 10 years of work experience in clinical nursing or infection control; bachelor’s degree or above; intermediate or higher professional nurse titles. After the interview and consultation with the 6 experts, the researchers created the work interruption survey, which had 11 items. The survey collected information on negative experiences and work interruption that had occurred during the past week. Negative experiences of the frontline nurses included 3 dimensions: frequency, severity, and distress. Incidence of work interruptions were scored as follows: Work interruption and negative experiences were scored with yes or no questions (yes=1, no=0); the frequency and severity of occurrence were scored on a Likert 3-level scoring method (1=occasionally/slightly, 2=sometimes/moderate, 3=often/severe); and the degree of disturbance was scored on a Likert 4-level scoring method (0=no disturbance, 1=mild, 2=moderate, 3=severe). If there were no negative experiences, the score was 0. If there were negative experiences, the participants were required to complete 11 items. For each item, there were 3 dimensions: frequency of occurrence (score of 0–3), severity (score of 0–3), and degree of disturbance (score of 0–3). The highest score for each item was 9. The total scores of negative experiences ranged from 0 to 99, with a higher score indicating the nurse experienced a more severe negative experience.
DATA COLLECTION PROCEDURE:
WeChat was the online medium used to send questionnaires to participants. WeChat was used to collect questionnaire data, and each item was set as mandatory (questionnaire generation link:
STATISTICAL ANALYSIS:
SPSS version 19.0 was used for the statistical analysis. The continuous data were expressed by mean±standard deviation, and the categorical data were expressed by frequency and percentage. The negative experience score was a continuous variable, and the remaining items were categorical binary variables. The chi-squared test,
Results
GENERAL INFORMATION:
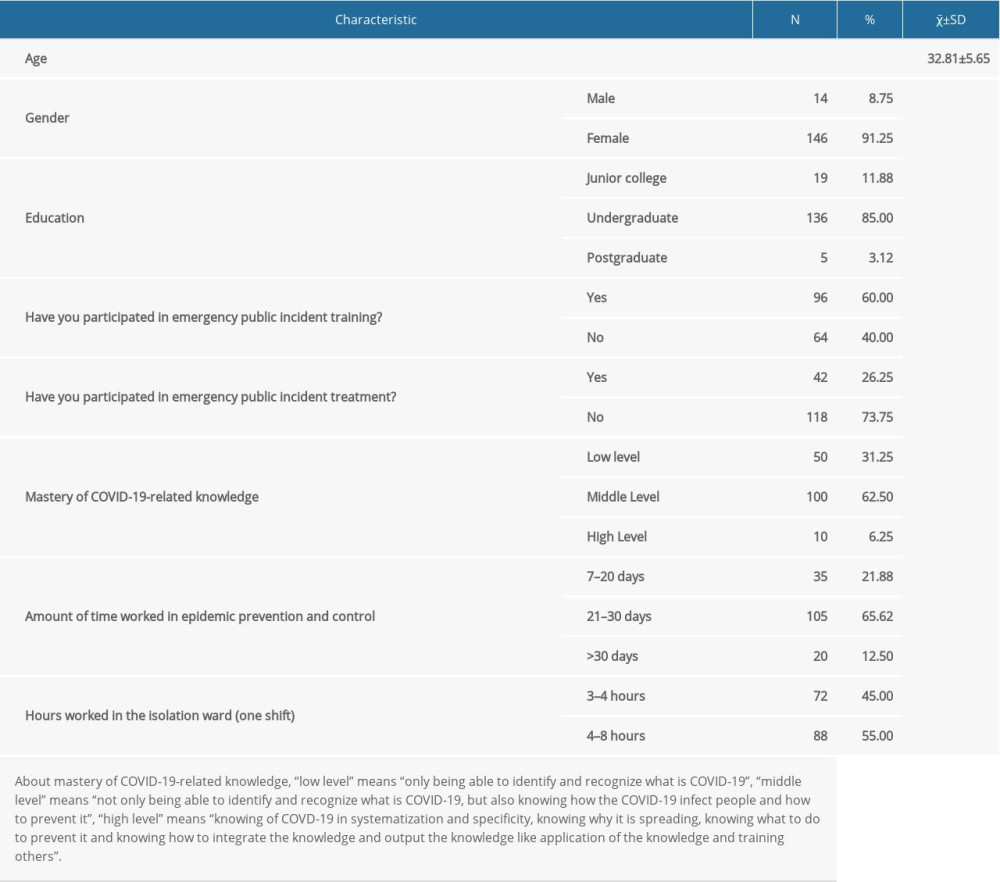
There were a total of 160 nurses from the working isolation wards, including Sino-French New City Campus of Tongji Medical College of HUST, Taikang Tongji (Wuhan) Hospital, and Huoshenshan Hospital, included in this survey. The nurses included 14 men (8.75%) and 146 women (91.25%), with the following demographics: age range of 24 to 49 years (32.8±5.6 years); education level included 19 junior college students (11.88%), 136 undergraduates (85.0%), and 5 master’s level (3.12%); 96 had participated in emergency public incident training (60.0%) and 64 (40.0%) did not; 42 (26.25%) participated in emergency public incident treatment and 118 (73.75%) did not; 50 (31.25%) had a low level of knowledge about COVID-19, 100 (62.5%) had a middle level of knowledge about COVID-19, and 10 (6.25%) had a high level of knowledge about COVID-19; 35 (21.88%), 105 (65.62%), and 20 (12.50%) worked in epidemic prevention and control for 7 to 20, 21 to 30, >30 days, respectively; and 72 (45.00%) and 88 (55.00%) worked 3 to 4 h and 5 to 8 h per shift in an isolation ward, respectively (Table 1).
CURRENT SITUATION AND NEGATIVE EXPERIENCES OF WORK INTERRUPTION:
In the study, the total score of negative experiences among clinical frontline nurses working to treat, prevent, and control the COVID-19 pandemic was 20.36±14.09 points; the scores of the 3 dimensions of negative experiences, frequency, severity, and distress, were 6.98±4.46, 6.89±4.91, and 6.50±5.73 points, respectively. During the COVID-19 epidemic, 25.0% of nurses in isolation wards had experienced work interruptions in the previous week and up to 96.87% of nurses had negative work experiences (Table 2).
ANALYSIS OF WORK INTERRUPTION IN ISOLATION WARDS OF CLINICAL FRONTLINE NURSES:
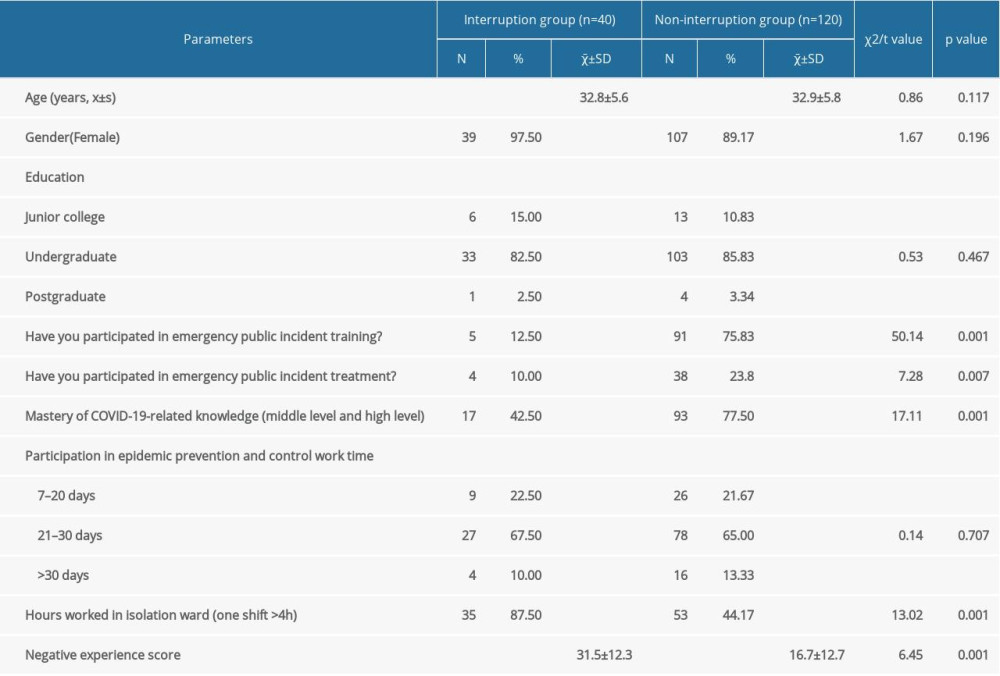
In the group of 120 nurses whose work was not interrupted (non-interruption group), 91 nurses (75.83%) had participated in emergency public incident training, 42 (26.25%) had participated in emergency public incident treatment, and 93 (77.50%) had a middle or higher knowledge level of COVID-19 (Table 3). The results of the univariate analysis showed that emergency public incident training, emergency public incident treatment experience, and COVID-19-related knowledge led to few interruptions. In this non-interruption group, 53 (44.17%) nurses worked over 4 h for 1 shift compared with 35 (87.5%) in the interruption group. Negative physiologic experience scores were 16.7±12.7 in the non-interruption group and 31.5±12.3 in the interruption group (Table 3). The results showed that the hours of continuous work and negative physiologic experiences may have affected the occurrence of interruptions.
LOGISTIC REGRESSION ANALYSIS OF WORK INTERRUPTION IN ISOLATION WARDS OF CLINICAL FRONTLINE NURSES:
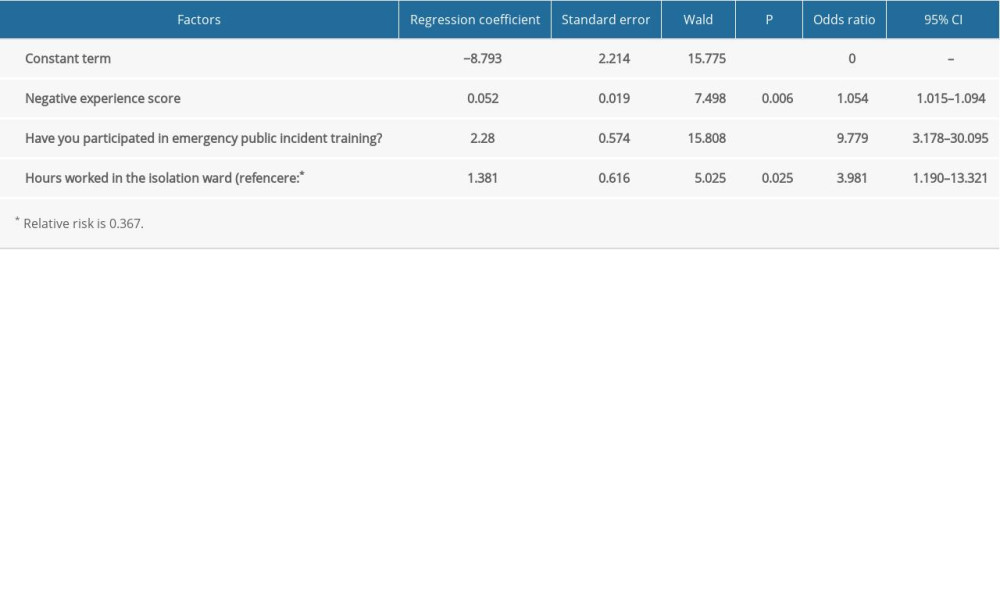
Regression analysis was performed with the occurrence of work interruption as the dependent variable and with the factors with statistical differences in the univariate analysis as the independent variables. The results showed that hours worked in isolation wards, whether a nurse had participated in emergency public incident training, and the negative experience score were independent factors influencing the interruption of nurses’ work in isolation wards (Table 4). When the negative experience score was higher, the incidence of work interruption was higher, which we interpreted to indicate that negative experience contributed to uncomfortable feelings both psychologically and physically. The incidence of work interruption was lower among those who had participated in public incident training, which may indicate that these nurses could grasp more relevant knowledge and experience about the emergency situation, were more familiar with the process and precautions of working in the emergency situation, and had stronger psychological endurance than those who did not participate emergency training. When the working hours of each shift were longer, the incidence of work interruption was higher, indicating that the nurses may have been uncomfortable from the heat created by wearing the protective clothing, may have had increased sweating and loss of electrolytes, and may have had headaches and nausea caused by wearing the masks and goggles, which created pressure on the face and head.
Discussion
CURRENT SITUATION OF WORK INTERRUPTION AMONG NURSES IN ISOLATION WARDS:
In each shift with an average length of 7 h 12 min in surgical wards, interruptions occurred 40.3 times on average in an observational study [11], which indicated that work interruptions among nurses are common. The interruptions also relate to the patient and severity of a task and its urgency [12]. Serious reduction of work efficiency can occur in nurses when dealing with intensive care work [5]. Isolation wards are highly intensive care units, which demand the conduct of tasks with a high level of urgency and severity in different kinds of patients, leading to nurses experiencing work interruptions. In the present study, 40 of 160 nurses had experiences of interruptions, an occurrence rate as high as 25%. The higher the rate of participating in emergency public incident training and emergency public incident treatment and the more COVID-19-related knowledge the nurses had, the less the nurses reported interruptions (Table 3).
NEGATIVE EXPERIENCE AS AN INDEPENDENT FACTOR INFLUENCING WORK INTERRUPTION AND RECOMMENDED MEASURES:
Due to the multiple transmission routes of COVID-19 [13], medical staff were at high risk for infection during the diagnosis and treatment of patients with COVID-19; therefore, for safety reasons, they wore personal protective equipment for an extended time. During long shifts, the wearing of personal protective equipment causes adverse effects on medical workers, including increased heat, thirst, pressure areas, headaches, and extreme exhaustion, as well as the inability to use the bathroom [14]. The present study found that the most common negative experiences among nurses in isolation wards were headaches, dyspnea, shortness of breath, and palpitations (Table 2). Also, the isolation wards needed to be disinfected multiple times throughout the day to prevent environmental contamination and reduce infections [15], which could cause adverse reactions and physical injury to the medical staff after long-term exposure to alcohol, chlorine-containing disinfectants, or other disinfectant substances [16]. Therefore, the nurses should be trained on how to use personal protective equipment correctly. Disinfectants should be correctly configured with a standardized concentration, their use should be optimized, and the exposure time of personnel in the environment of disinfectants should be reduced.
Biological occupational exposure also led to negative experiences and a high incidence of work interruptions among nurses in isolation wards [17,18]. Occupational biological exposure of medical staff refers to the possibility of contamination of the skin and mucous membranes with blood, body fluids, and excreta from carriers of infectious pathogens during diagnosis, treatment, and nursing activities [18]. In special working environments like COVID-19 isolation wards, if a nurse were experiencing severe negative experiences, but insisted on working, it would pose a great threat to the nurse’s physical and mental health.
In this study, negative experience was shown to be an independent factor influencing work interruptions among nurses in isolation wards. The nurses were under pressure from a high risk of infection, insufficient rest time, and working with intensity in difficult circumstances. Our results showed that the nurses experienced uncomfortable symptoms, such as dizziness, headaches, and shortness of breath (Table 2). Negative physiologic experience scores in the non-interruption group were lower than those in the interruption group (Table 3). Thus, negative experience was an independent factor influencing work interruption. In the future, it is imperative to ensure that medical personnel in a high-risk exposure group are given reasonable rest periods, correct instruction in the use of personal protective equipment, and less exposure to disinfectants, as well as other measures to protect the occupational health and safety of medical personnel.
WORKING HOURS AS AN INDEPENDENT FACTOR INFLUENCING WORK INTERRUPTION AND RECOMMENDED MEASURES:
The results of this study suggested that working over 4 h was an independent risk factor for nurse interruptions while working in isolation wards. During the COVID-19 pandemic, there were many severely ill patients in isolation wards, the workload of nurses increased sharply, and the psychological load was heavier than that of non-epidemic periods [19]. The increased working hours per shift can cause nurses to be physically and mentally exhausted, leading to frequent work interruptions [19,20]. The long working hours of nurses can negatively impact the positive patient safety culture, which is one of the most critical components to improve healthcare quality and safety [21]. During the epidemic, nursing staff were faced with high-intensity multitasking work during each shift. Each additional hour worked meant that the nurse needed to increase the load of multitasking hours, increasing the possibility that care interruption will be increased. Thus, working hours need to be properly arranged, and adjustments should be made in consideration of the physical and mental capacity of the nurses to ensure a 4-h shift system, which may effectively reduce the interruption of nursing duties.
EMERGENCY PUBLIC INCIDENT TRAINING AS AN INDEPENDENT FACTOR INFLUENCING WORK INTERRUPTION AND RECOMMENDED MEASURES:
Emergency public incident training is an independent factor influencing work interruption among nurses in isolation wards [22]. During the outbreak of a large-scale epidemic, training of various nursing theories and skills are particularly important [23]. The training content mainly includes self-protection knowledge and skills, professional knowledge and skills, and preventive psychological counseling [23]. Emergency public incident training is an important way for nurses to acquire knowledge and skills related to emergency public incidents, by which nurses can improve their ability to respond to those incidents [24,25]. The COVID-19 epidemic occurred suddenly and required medical staff to be prepared physically and psychologically. A previous study showed that the lack of mental preparation and mental overload of nursing staff are closely related to interruption of nursing care and decreased satisfaction with nursing services [26]. Scene simulation training can cultivate the ability of junior emergency nurses to deal with various emergent problems and improve communication skills, learning ability, and cooperation with doctors and effectively improve their working ability [27]. Therefore, practical training should be widely used in combination with theoretical training.
The results of the present study showed that during the epidemic, nurses lacking emergency public incident training were more likely to experience work interruptions, which reduced work efficiency, than those who had received relevant training. We should therefore prepare for emergencies, reduce the lack of preparedness due to panic and a lack of knowledge, thereby reducing the occurrence of work interruptions and protecting the physical and mental health of medical workers.
LIMITATIONS:
This study had some limitations. The sample size was small, and further study should be performed in multiple centers to verify our results. Owing to the epidemic, the questionnaire was an online survey, and we had pre-designed the range of answers, which limited the respondents’ answers and therefore may have missed more detailed information. The survey parameters of the questionnaire were limited, and more parameters need to be considered in the future.
Conclusions
In the study, the incidence rate of work interruption among nurses in isolation wards was 25%, and many types of negative physiologic experiences occurred. The analysis of the factors influencing work interruption among nurses showed that the working hours for each shift, emergency public event (treatment) training, and negative physiologic experiences were independent factors for nurses’ work interruptions. Therefore, the education of nurses in relevant knowledge and practical training should be increased before they participate in the treatment of such public incidents, and the working hours of each shift should be reasonably arranged to strengthen the monitoring of negative physiologic experiences and reduce work interruptions.

References
1. Li Q, Guan X, Wu P, Early transmission dynamics in Wuhan, China, of novel coronavirus – infected pneumonia: N Engl J Med, 2020; 382(13); 1199-207
2. Chan JF, Yuan SF, Kok KH, A familial cluster of pneumonia associated with the 2019 novel coronavirus indicating person-to-person transmission: Astudy of a family cluster: Lancet, 2020; 395(10223); 514-23
3. Sang H, Cui Y, Lai X, A familial cluster of coronavirus disease 2019 (COVID-19) caused by one family member during his asymptomatic incubation period: J Public Health (Oxf), 2020; 42(3); 656-58
4. Turale S, Meechamnan C, Kunaviktikul W, Challenging times: Ethics, nursing and the COVID-19 pandemic: Int Nurs Rev, 2020; 67(2); 164-67
5. Drews FA, Markewitz BA, Stoddard GJ, Interruptions and delivery of care in the intensive care unit: Hum Factors, 2019; 61(4); 564-76
6. Forsyth KL, Hawthorne HJ, El-Sherif N, Interruptions experienced by emergency nurses: Implications for subjective and objective measures of workload: J Emerg Nurs, 2018; 44(6); 614-23
7. Reed CC, Minnick AF, Dietrich MS, Nurses’ responses to interruptions during medication tasks: A time and motion study: Int J Nurs Stud, 2018; 82; 113-20
8. Bellandi T, Cerri A, Carreras G, Interruptions and multitasking in surgery: A multicentre observational study of the daily work patterns of doctors and nurses: Ergonomics, 2018; 61(1); 40-47
9. Wang Q, Guo JY, Sun HInvestigation of protective exposure risk events in nurses against corona virus disease 2019 in Wuhan: Beijing Da Xue Bao Yi Xue Ban, 2020; 52(4); 711-14 [in Chinese]
10. McCurdie T, Sanderson P, Aitken LM, Traditions of research into interruptions in healthcare: A conceptual review: Int J Nurs Stud, 2017; 66; 23-36
11. Dante A, Andrigo I, Barone F, Occurrence and duration of interruptions during nurses’ work in surgical wards: Findings from a multicenter observational study: J Nurs Care Qual, 2016; 31(2); 174-82
12. Sasangohar F, Donmez B, Easty A, The relation between interruption content and interrupted task severity in intensive care nursing: An observational study: Int J Nurs Stud, 2015; 52(10); 1573-81
13. Naserghandi A, Allameh SF, Saffarpour R, All about COVID-19 in brief: New Microbes New Infect, 2020; 35; 100678
14. Tabah A, Ramanan M, Laupland KB, Personal protective equipment and Intensive Care Unit healthcare worker safety in the COVID-19 era (PPE-SAFE): An international survey: J Crit Care, 2020; 59; 70-75
15. Ye G, Lin H, Chen S, Environmental contamination of SARS-CoV-2 in healthcare premises: J Infect, 2020; 81(2); e1-5
16. Sharafi SM, Ebrahimpour K, Nafez A, Environmental disinfection against COVID-19 in different areas of health care facilities: A review: Rev Environ Health, 2020 [Online ahead of print]
17. Chen SL, Chen KL, Lee LH, Working in a danger zone: A qualitative study of Taiwanese nurses’ work experiences in a negative pressure isolation ward: Am J Infect Control, 2016; 44(7); 809-14
18. Oh HS, Uhm DC, Occupational exposure to infection risk and use of personal protective equipment by emergency medical personnel in the Republic of Korea: Am J Infect Control, 2016; 44(6); 647-51
19. Aksoya YE, Koçakb V, Psychological effects of nurses and midwives due to COVID-19 outbreak: The case of Turkey: Arch Psychiatr Nurs, 2020; 34(5); 427-33
20. Fernandez PR, Lord H, Halcomb PE, Implications for COVID-19: A systematic review of nurses’ experiences of working in acute care hospital settings during a respiratory pandemic: Int J Nurs Stud, 2020; 111; 103637
21. Wu YH, Fujita S, Seto K, The impact of nurse working hours on patient safety culture: A cross-national survey including Japan, the United States and Chinese Taiwan using the Hospital Survey on Patient Safety Culture: BMC Health Serv Res, 2013; 13; 394
22. Middleton A, 405-O. Emergency preparedness training – Emergency and community nurses’ perceived needs: J Emerg Nurs, 2006; 32(4); 274
23. Mugford B, Martin A, Owen H, Simulation training in emergency medicine. An important need for primary care training: Aust Fam Physician, 2004; 33(4); 279-80
24. Labrague LJ, Yboa BC, McEnroe-Petitte DM, Disaster preparedness in Philippine nurses: J Nurs Scholarsh, 2016; 48(1); 98-105
25. Thobaity AA, Plummer V, Innes K, Perceptions of knowledge of disaster management among military and civilian nurses in Saudi Arabia: Australas Emerg Nurs J, 2015; 18(3); 156-64
26. Westbrook JI, Duffield C, Li L, How much time do nurses have for patients? a longitudinal study quantifying hospital nurses’ patterns of task time distribution and interactions with health professionals: BMC Health Serv Res, 2011; 11; 319
27. Zhong LJ, Feng JH, Yu YApplication and clinical value of scene simulation training in first-aid skills training for junior emergency nurses: China Medicine and Pharmacy, 2019; 23; 38-40 [in Chinese]
In Press
Clinical Research
Institutional and Regional Variations in Access to Clinical Trials and Next-Generation Sequencing in Turkis...Med Sci Monit In Press; DOI: 10.12659/MSM.951027
Clinical Research
Low-Intensity Blood Flow-Restricted Multi-Joint Exercise Improves Muscle Function in Patients With Patellof...Med Sci Monit In Press; DOI: 10.12659/MSM.950516
Review article
Musculoskeletal Ultrasound and MRI in the Evaluation of Chemotherapy-Induced Peripheral Neuropathy: A ReviewMed Sci Monit In Press; DOI: 10.12659/MSM.951283
Clinical Research
Sensory Processing, Dissociation, and Affective Symptoms in Misophonia: A Cross-Sectional Study of 35 AdultsMed Sci Monit In Press; DOI: 10.12659/MSM.950938
Most Viewed Current Articles
17 Jan 2024 : Review article 10,187,196
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,708,487
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,341,643
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 706,524
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387