21 December 2020: Clinical Research
Retrospective Study of Clinical Features of COVID-19 in Inpatients and Their Association with Disease Severity
Hao Wang1AE, Yang Xing2CDEF, Xiaohong Yao3BD, Yang Li1C, Jietao Huang1CD, Jun Tang1BF, Shasha Zhu1CD, Ying Zhang1EG, Jun Xiao1G*DOI: 10.12659/MSM.927674
Med Sci Monit 2020; 26:e927674






Abstract
BACKGROUND: The aim of this study was to analyze the clinical features and laboratory indices of patients with coronavirus disease (COVID-19) and explore their association with the severity of the disease.
MATERIAL AND METHODS: A total of 61 patients with COVID-19 were divided into groups with common symptoms and with severe diseases, and clinical data were collected to analyze and compare the differences between them.
RESULTS: In patients with severe COVID-19, compared with the common group, lymphocyte count and albumin levels were lower, and aspartate aminotransferase (AST), blood urea, blood creatinine, lactate dehydrogenase (LDH), and C-reactive protein (CRP) levels, and prothrombin time (PT) were elevated (all P<0.05). The neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), mean platelet volume-to-lymphocyte ratio (MPVLR), and C-reactive protein-to-albumin ratio (CAR) were significantly elevated in the severe group compared with the group with common symptoms; however, the lymphocyte-to-monocyte ratio (LMR) was significantly reduced (P<0.05). Univariate logistic regression showed that lower lymphocyte count, prolonged PT, elevated CRP and LDH levels, and elevated NLR, PLR, MPVLR, and CAR were risk factors for COVID-19 severity (P<0.05). Multivariate logistic regression showed that elevated CRP levels (odds ratio [OR], 0.028; 95% confidence interval [CI]: 0.002–0.526; P=0.017), prolonged PT (OR, 0.014; 95% CI: 0.001–0.341; P=0.09), and an MPVLR >8.9 (OR, 0.026; 95% CI: 0.002–0.349; P=0.006) were independent risk factors for COVID-19 severity.
CONCLUSIONS: Elevated CRP and prolonged PT, and an MPVLR >8.9 were independent risk factors for COVID-19 severity.
Keywords: COVID-19, Medical Informatics, Nutrition Assessment, Aspartate Aminotransferases, Blood Platelets, C-Reactive Protein, COVID-19, Coronavirus, Coronavirus Infections, Creatinine, Inpatients, L-Lactate Dehydrogenase, Lymphocyte Count, Lymphocytes, mean platelet volume, Monocytes, Neutrophils, SARS-CoV-2, Serum Albumin, Severity of Illness Index
Background
Coronavirus disease 2019 (COVID-19) is an infectious disease caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). It primarily presents with respiratory symptoms caused by inflammatory lesions of the lungs and can result in damage to the digestive, nervous, and cardiovascular systems. Because the disease progresses rapidly, it can lead to multiple organ failure and even death [1]. Currently, the COVID-19 pandemic is a global health threat, and the infection rate outside China has increased rapidly. To date, more than 5 million cases of COVID-19 have been diagnosed globally, with a high mortality rate. Previous studies have shown that early identification and treatment of patients with severe COVID-19 can have a positive impact on blocking the progression and improving the outcome of the disease. Therefore, determining disease severity at an early stage is crucial for better outcomes. In this study, to guide early detection, diagnosis, and treatment of severe cases, we retrospectively analyzed the general condition of, clinical symptoms and signs in, and blood test results from 61 patients with newly diagnosed COVID-19 who were admitted to the isolation ward of Dawu Hospital of Traditional Chinese Medicine in Xiaogan City, Hubei Province.
Material and Methods
SUBJECTS:
This was a retrospective study. Sixty-one patients with confirmed COVID-19 who were admitted to the isolation ward of the Dawu Hospital of Traditional Chinese Medicine in Xiaogan City, Hubei Province, from January 23 to March 11, 2020, were enrolled. The diagnoses were made based on positive results for COVID-19 nucleic acids on real-time fluorescence reverse transcription-polymerase chain reaction (RT-PCR), as described in the Diagnosis and Treatment Protocol for Novel Coronavirus Pneumonia (Trial Version 7) [2].
The study was performed with the approval of the Chongqing University Center Hospital Ethics Committee (Ethics No. 17, 2020). Verbal consent was provided by all patients, but the requirement for written informed consent was waived, given the state of an emerging infectious disease.
DEFINITIONS:
The patients were divided into 2 groups: a group that included 37 cases that were mild and associated with common symptoms, and another that included 24 cases that were severe and critical. The classification criteria were based on the Diagnosis and Treatment Protocol for Novel Coronavirus Pneumonia (Trial Version 7) released by the General Office of the National Health Commission of China [2]. The specific clinical types included were: 1. Mild (mild clinical symptoms with no sign of pneumonia on imaging); 2. Common (fever, respiratory tract infection, and imaging indicative of pneumonia); 3. Severe (respiratory distress and respiratory rate (RR) ≥30 breaths/min or oxygen saturation ≤93% at rest, or partial pressure of oxygen [PaO2]/fraction of inspired oxygen [FiO2] ≤300 mmHg [1 mmHg=0.133 kPa]); and 4. Critical (respiratory failure and a requirement for mechanical ventilation or shock or concomitant failure of other organs and requirement for intensive care unit monitoring and treatment).
RESEARCH METHODS:
Age, sex, comorbidities, clinical symptoms, vital signs, and laboratory indices, such as results of routine blood tests, liver and kidney function, coagulogram, myocardial enzymes, blood lipids, C-reactive protein (CRP), procalcitonin (PCT), and other markers that might reflect disease conditions were retrospectively analyzed in the 2 groups. Studies have suggested that the neutrophil-to-lymphocyte ratio (NLR), lymphocyte-to-monocyte ratio (LMR), platelet-to-lymphocyte ratio (PLR), mean platelet volume-to-lymphocyte ratio (MPVLR), C-reactive protein-to-albumin ratio (CAR), and other peripheral blood cell inflammatory markers could serve as indices for evaluating the severity of multisystem diseases, including infectious diseases) [3–6]. Therefore, we calculated these ratios and compared differences in them between the 2 groups.
STATISTICAL ANALYSIS:
Categorical variables were described as frequency rates and percentages, and continuous variables were described using mean, median, and interquartile range (IQR) values. Means for continuous variables were compared using independent group
Results
GENERAL CHARACTERISTICS AND CLINICAL PRESENTATIONS:
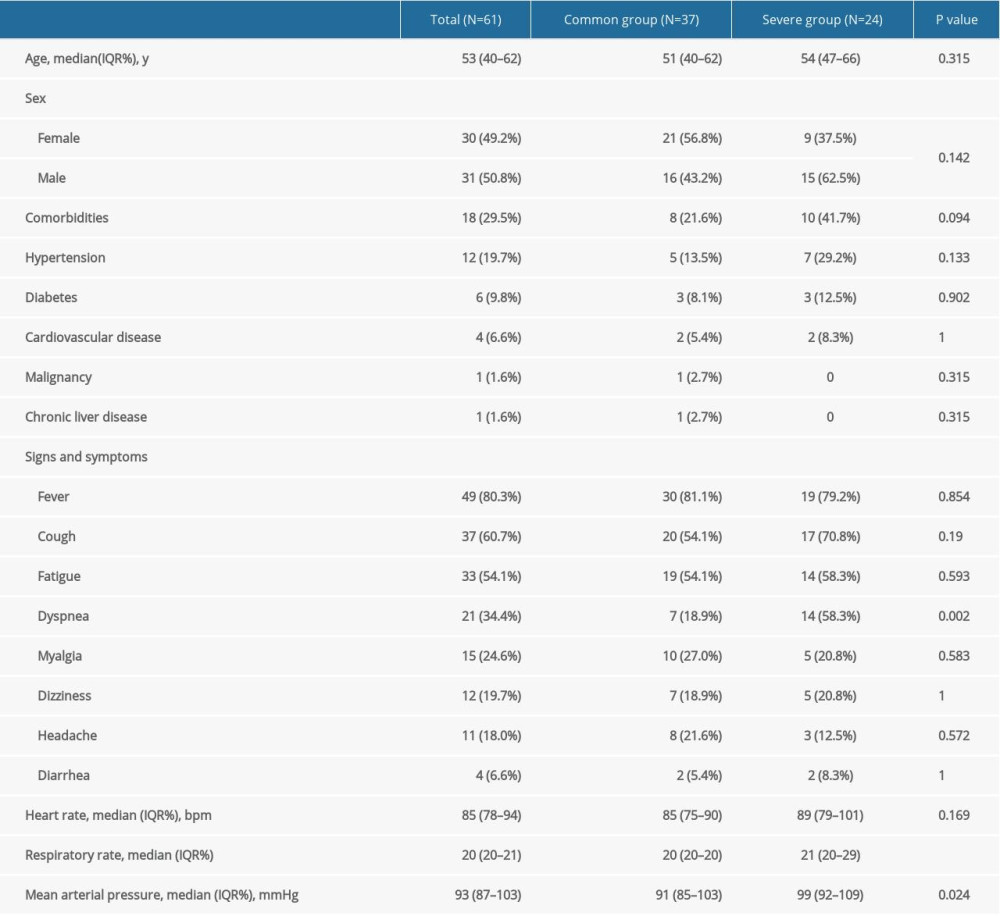
Among the 61 patients, 37 were in the common group (mild and common disease severity), and 24 were in the severe group (severe and critical disease severity). The median age of all the patients was 53 years (IQR 35.0–62.0), and was not significantly different between the common and severe groups (ages 51 and 54 years, respectively). Of the 61 patients, 30 were female (49.2%), and 31 were male (50.8%). There were 21 females (56.8%) and 16 males (43.2%) in the common group and 9 females (37.5%) and 15 males (62.5%) in the severe group (P>0.05). There were 18 patients (29.5%) with various comorbidities, including 12 with hypertension (19.7%), 6 with diabetes (9.8%), 4 with cardiovascular disease (6.6%), 1 with a malignant tumor (1.6%), and 1 with chronic liver disease (1.6%). The difference between the 2 groups in the proportion of each disease was not statistically significant (P>0.05). The common symptoms in the enrolled patients were fever (49 cases, 80.3%) and cough (37 cases, 60.7%), followed by fatigue (33 cases, 54.1%), dyspnea (21 cases, 34.4%), and myalgia (15 cases, 24.6%); some patients were admitted to the hospital with dizziness, headache, diarrhea, and other symptoms. The proportion of patients admitted to the hospital due to dyspnea in the severe group (14 cases, 58.3%) was significantly higher than that in the common group (7 cases, 18.9%). The difference between the 2 groups was significant (P=0.002). There were no significant differences in heart rate or mean arterial pressure between the 2 groups at admission, but the respiratory rate was significantly higher in the severe group than in the common group (21 [IQR 20–29] vs. 20 [IQR 20–20], P=0.004) (Table 1).
COMPARISON OF LABORATORY INDICES BETWEEN THE 2 GROUPS:
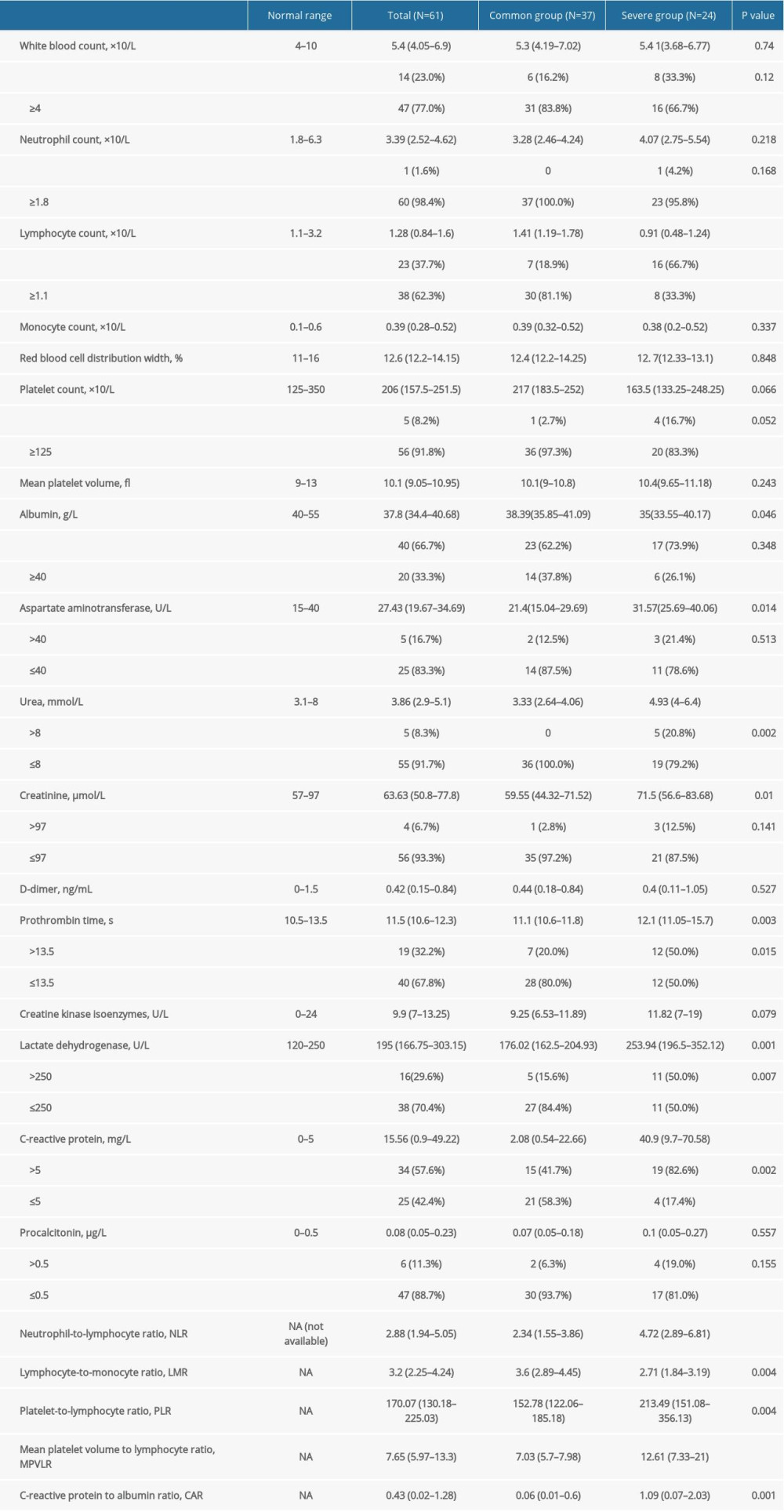
There were more differences in the laboratory findings of patients at admission between the severe and common groups. In the severe group, compared with the common group, lymphocyte count and albumin levels were lower; however, aspartate aminotransferase (AST), blood urea, and blood creatinine levels were elevated, and PT was prolonged (P<0.05). The incidence of decreased lymphocyte count, elevated blood urea nitrogen blood creatinine levels, and prolonged PT was higher in the severe group than in the common group (P<0.05). There were no significant differences in white blood cell, neutrophil, or monocyte counts; red blood cell distribution width; platelet count; mean platelet volume; D-dimer; or creatine kinase isoenzyme between the 2 groups. In terms of inflammation indicators, the proportion and degree of elevated lactate dehydrogenase (LDH) and CRP in the severe group were greater than in the common group, and the differences were significant. However, there was no significant difference in procalcitonin between the 2 groups. Further, the differences in the ratios of peripheral blood cell inflammatory markers, such as NLR, LMR, PLR, MPVLR, and CAR, in the 2 groups also were assessed. Compared with the common group, in the severe group, the NLR, PLR, MPVLR, and CAR were significantly elevated; however, the LMR was significantly decreased (P<0.05) (Table 2).
LOGISTIC REGRESSION OF FACTORS AFFECTING COVID-19 SEVERITY:
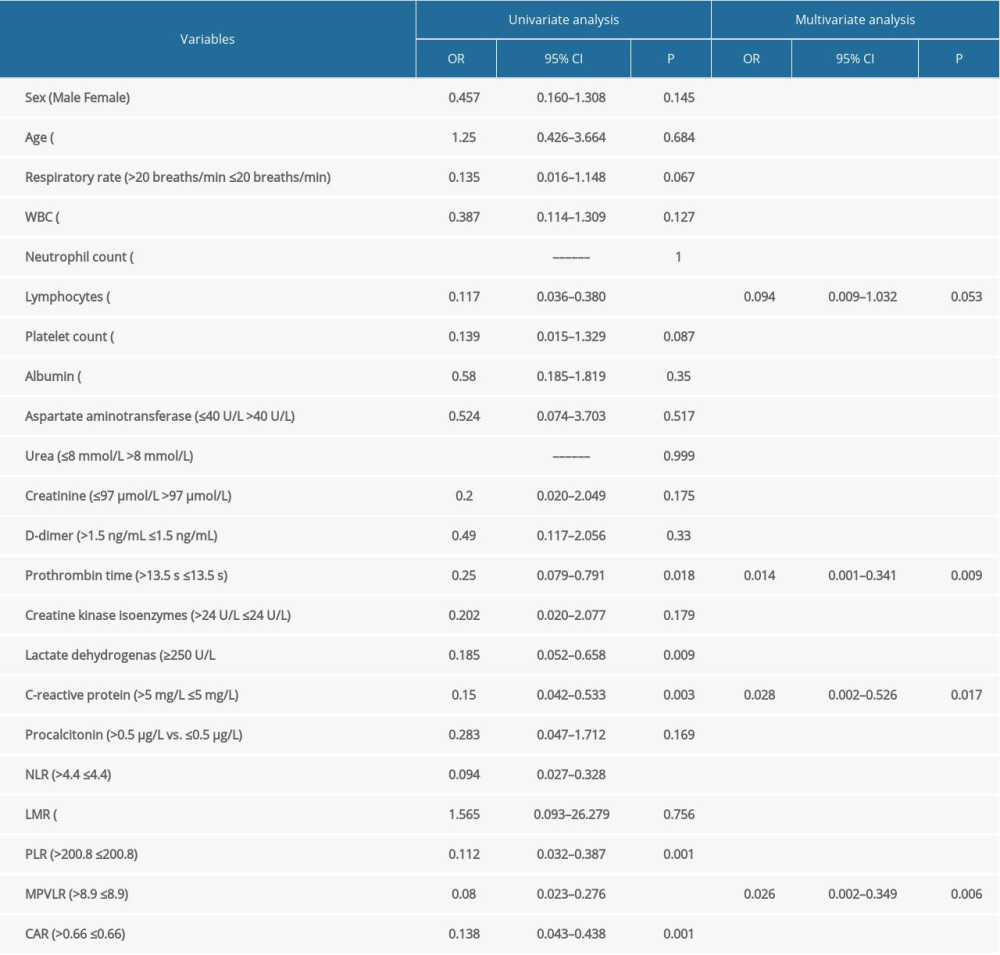
Based on clinical experience and previous research conclusions, we conducted receiver operating characteristic analysis of the above ratios and obtained the cut-off value, which was set as the limit. Measurement data for the ratios were converted into count data, which were then included in the logistic regression. Univariate logistic regression showed that decreased lymphocyte count (OR, 0.117; 95% confidence interval [CI]: 0.036–0.380; P<0.001), elevated CRP (OR, 0.150; 95% CI: 0.042–0.533; P=0.003) levels, elevated LDH (OR, 0.185; 95% CI: 0.052–0.658; P=0.009), prolonged PT (OR, 0.250; 95% CI: 0.079–0.791; P=0.018), NLR >4.4 (OR, 0.094; 95% CI: 0.027–0.328; P<0.001), PLR >200.8 (OR, 0.112; 95% CI: 0.032–0.387; P=0.001), MPVLR >8.9 (OR, 0.08; 95% CI: 0.023–0.276; P<0.53001), and CAR >0.0966 (OR, 0.438; 95% CI: 0.043–0.438; P=0.001) were risk factors for COVID-19 severity (P<0.05). In the univariate analysis, the effect of factors can be affected by other factors and show statistical significance, but it may not be a result of the factor itself. In this case, multivariate analysis may conclude that a factor is not statistically significant. The statistically significant parameters in the univariate analysis (P<0.05) were all included in the multivariate logistic regression. The backward Wald method was used for parameter selection. Four factors – LDH, NLR, PLR, and CAR – were excluded during the selection. The remaining factors – lymphocyte count CRP, PT, and MPVLR – were included into the final multivariate logistic regression model. The results suggested that elevated CRP (OR, 0.028; 95% CI: 0.002–0.526; P=0.017), prolonged PT (OR, 0.014; 95% CI: 0.001–0.341; P=0.09), and MPVLR >8.9 (OR, 0.026; 95% CI: 0.002–0.349; P=0.006) were independent risk factors for COVID-19 severity (Table 3).
Discussion
COVID-19 is rapidly progressive. A few patients have been observed to develop of acute respiratory distress syndrome (ARDS), shock, and severe coagulation dysfunction over a short period of time and then die due to systemic inflammatory response syndrome (SIRS) [1]. Currently, there is no effective treatment for COVID-19. However, the mortality rate can be reduced by understanding the risk factors for disease severity and taking active and beneficial measures.
Among the 61 patients enrolled, the median age was 53 years (IQR 35.0–62.0). In individuals at this age, working and participating in social activities such as parties can contribute to increased risk of contracting COVID-19. Men are more frequently reported to be infected with it than women [7], and older men (>60 years) with comorbidities are more likely to develop ARDS [8]. There were no significant differences in age, sex, or comorbidities between the 2 groups in this study, possibly due to the small sample size. Further observation and research are required to determine how these factors affect disease severity.
The common symptoms seen in patients at the initial onset of COVID-19 infection are fever, cough, and fatigue, followed by dyspnea, myalgia, dizziness, headache, and diarrhea. Our findings were consistent with other studies [9,10]. Because the virus primarily invades the respiratory system, patients in the severe group were more prone to develop dyspnea and an increased respiratory rate. Therefore, respiratory indices are particularly important for evaluating the severity of COVID-19.
In this study, lymphocyte count and albumin levels were decreased; AST, blood urea, blood creatinine, LDH, and CRP levels were elevated; and PT was prolonged in the severe group compared with the common group, which is consistent with the findings observed in patients with MERS-COV and SARS-COV infections [11], and most patients with COVID-19 [8–10]. The regression analysis showed that reduced lymphocyte counts, elevated CRP and LDH levels, and prolonged PT are related to the severity of the disease. Aggravated SARS-CoV-2 infection is associated with cellular immune deficiency, systemic inflammatory response, coagulation activation, liver and kidney injury, and myocardial injury. Some studies have shown that patients with severe COVID-19 have elevated D-dimer levels compared with individuals with common cases [1,10,12]. However, this difference was not observed in the present study, which may be related to its sample size.
Several studies have reported that the ratios of peripheral blood-related parameters, such as NLR, LMR, PLR, MPVLR, and CAR, which are new inflammatory indices, are beneficial in evaluating the severity of multisystem diseases, including infectious diseases [3–6]. In this study, these ratios were significantly different between the 2 groups, and the regression analysis suggested that they are related to disease severity. These ratios might be associated with increased immunosuppression and inflammation in severe cases. The NLR and PLR have been reported to be possibly related to the severity of COVID-19 [13,14]. However, the ratios of the remaining parameters have not been reported in the analysis of patients with COVID-19.
The multivariate logistic analysis showed that elevated CRP, prolonged PT, and MPVLR >8.9 were independent risk factors for COVID-19 severity. CRP, a nonspecific reactive protein produced by liver cells, participates in various inflammatory reactions in the body, activates the complement system, promotes phagocytosis, and regulates immunity. It is currently the clinical sensitivity index most commonly used to reflect the degree of infection. COVID-19 infection triggers a systemic inflammatory response. Several studies have reported that elevated CRP is associated with severe COVID-19 [8–10], which is consistent with the findings of the present study. PT is a test used to diagnose bleeding or clotting disorders in the exogenous coagulation system. Previous studies have suggested that PT is prolonged in severe COVID-19 cases [10,13]. This study further demonstrated that PT is an independent risk factor for COVID-19 severity. The etiology may be that hypoxia and toxins in severe pneumonia inflict vascular endothelial damage on the body, promote the release of inflammatory mediators such as prostaglandin A2 and histamine, and cause platelet aggregation, arteriospasm, and microvascular thrombosis with excessive consumption of coagulation factors. Also, coagulation can be considered another line of defense against serious infections, given its role in immune function [15]. Therefore, monitoring blood coagulation is important for judging the severity of COVID-19.
Recently, MPVLR has emerged as a new inflammatory parameter. Several studies have shown that it has predictive value for the diagnosis and prognosis of cardiovascular and cerebrovascular diseases, diabetes, kidney and liver disease, and appendicitis [16–20]. However, no relevant research has been conducted on the value of MPVLR for diagnosing and predicting the severity of COVID-19 and other coronavirus infections. MPV can be used as a marker for the rate of platelet production and activation in the bone marrow [21]. In patients with severe pneumonia, the microvessel endothelium is damaged by inflammatory mediators, hypoxia, pathogens, and toxins released during reproduction, and platelets are activated in a hypercoagulable state, resulting in a significant increase in platelet consumption and a compensatory increase in bone marrow platelet volume. As a result, MPV is significantly elevated. Also, lymphocytes have been observed to decrease in patients with COVID-19, which is related to the severity of the disease. The reason may be that SARS-CoV-2 mainly acts on lymphocytes. The lymphocyte count of COVID-19 patients indicates the degree to which the coronavirus consumes immune cells and suppresses the body’s cellular immune function. When the disease progresses, and immune suppression worsens, the proportion of lymphocytes decreases significantly. Therefore, compared with the MPV or lymphocyte count alone, the MPVLR can reflect coagulation system abnormalities and immune system suppression, as well as the interaction between 2 different hemocyte cell lines. It can reflect systemic inflammation and severity better than a single indicator. In this study, the MPVLR was confirmed to be superior to MPV or lymphocytes alone through multivariate logistic regression analysis, and it was an independent risk factor for COVID-19 severity. An MPVLR >8.9 was considered to be a high risk for COVID-19 severity.
Conclusions
This study suggests that fever and cough are the main manifestations of COVID-19 in patients at diagnosis, and attention should be paid to patients with symptoms of dyspnea. Moreover, patients with elevated CRP, prolonged PT, and elevated MPVLR (>8.9) should be treated cautiously for prompt prevention of severe illnesses.
As a retrospective study, the data are true and reliable in this study. However, given the limitations of the small sample size and collection of data from a single center, the present research results should be interpreted cautiously. Multicenter clinical studies with larger sample sizes are required to confirm the findings.
References
1. Huang C, Wwang Y, Li X, Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China: Lancet, 2020; 395(10223); 497-506
2. , Diagnosis and treatment protocol for novel coronavirus pneumonia (Trial Version 7): China NHCOTPSRO 03 29, 2020 http://en.nhc.gov.cn/2020-03/29/c_78469.htm
3. Russell CD, Parajuli A, Gale HJ, The utility of peripheral blood leucocyte ratios as biomarkers in infectious diseases: A systematic review and meta-analysis: J Infect, 2019; 78(5); 339-48
4. Djordjevic D, Rondovic G, Surbatovic M, Neutrophil-to-lymphocyte ratio, monocyte-to-lymphocyte ratio, platelet-to-lymphocyte ratio, and mean platelet volume-to-platelet count ratio as biomarkers in critically ill and injured patients: Which ratio to choose to predict outcome and nature of bacteremia?: Mediators Inflamm, 2018; 2018; 3758068
5. Bozlu G, Karpuz D, Hallioglu O, Relationship between mean platelet volume-to-lymphocyte ratio and coronary artery abnormalities in Kawasaki disease: Cardiol Young, 2018; 28(6); 832-36
6. Oh J, Kim SH, Park KN, High-sensitivity C-reactive protein/albumin ratio as a predictor of in-hospital mortality in older adults admitted to the Emergency Department: Clin Exp Emerg Med, 2017; 4(1); 19-24
7. Chen N, Zhou M, Dong X, Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study: Lancet, 2020; 395(10223); 507-13
8. Liu W, Tao ZW, Lei W, Analysis of factors associated with disease outcomes in hospitalized patients with 2019 novel coronavirus disease: Chin Med J (Engl), 2020; 133(9); 1032-38
9. Long-quan L, Tian H, Yong-Qing W, COVID-19 patients’ clinical characteristics, discharge rate and fatality rate of meta-analysis: J Med Virol, 2020; 92(6); 577-83
10. Wang D, Hu B, Hu C, Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus-infected pneumonia in Wuhan, China: JAMA, 2020; 323(11); 1061-69
11. Gu J, Gong E, Zhang B, Multiple organ infection and the pathogenesis of SARS: J Exp Med, 2005; 202(3); 415-24
12. Wan S, Xiang Y, Fang W, Clinical features and treatment of COVID-19 patients in northeast Chongqing: J Med Virol, 2020; 92(7); 797-806
13. Qin C, Zhou L, Hu Z, The clinical features of the 143 patients with COVID-19 in North-East of Chongqing: Clin Infect Dis, 2020 [Online ahead of print]
14. Qu R, Ling Y, Zhang Y-H-Z, Platelet-to-lymphocyte ratio is associated with prognosis in patients with coronavirus disease-19: J Med Virol, 2020 [Online ahead of print]
15. Loof TG, Morgelin M, Johansson L, Coagulation, an ancestral serine protease cascade, exerts a novel function in early immune defense: Blood, 2011; 118; 2589-98
16. Bozlu G, Akar A, Durak F, Role of mean platelet volume-to-lymphocyte ratio in the diagnosis of childhood appendicitis: Arch Argent Pediatr, 2019; 117(6); 375-80
17. Coban E, Comment on “Mean platelet volume-to-lymphocyte ratio: A novel biomarker associated with overall survival in patients with nonmetastatic clear cell renal cell carcinoma treated with nephrectomy: ” Int Urol Nephrol, 2020; 52(9); 1703
18. Życzkowski M, Kaletka Z, Rajwa P, Prognostic value of pre-infarction angina combined with mean platelet volume to lymphocyte count ratio for no-reflow and short-term mortality in patients with ST-segment elevation myocardial infarction undergoing percutaneous coronary intervention: Med Sci Monit, 2020; 26; e919300
19. Chen SY, Lin YS, Cheng YF, Mean platelet volume-to-lymphocyte ratio predicts poor functional outcomes among ischemic stroke patients treated with intravenous thrombolysis: Front Neurol, 2019; 10; 1274
20. Hudzik B, Szkodziński J, Lekston A, Mean platelet volume-to-lymphocyte ratio: A novel marker of poor short- and long-term prognosis in patients with diabetes mellitus and acute myocardial infarction: J Diabetes Complications, 2016; 30(6); 1097-102
21. Ekiz F, Yuksel O, Kocak E, Mean platelet volume as a fibrosis marker in patients with chronic hepatitis B: J Clin Lab Anal, 2011; 25; 162-65
In Press
Clinical Research
Institutional and Regional Variations in Access to Clinical Trials and Next-Generation Sequencing in Turkis...Med Sci Monit In Press; DOI: 10.12659/MSM.951027
Clinical Research
Low-Intensity Blood Flow-Restricted Multi-Joint Exercise Improves Muscle Function in Patients With Patellof...Med Sci Monit In Press; DOI: 10.12659/MSM.950516
Review article
Musculoskeletal Ultrasound and MRI in the Evaluation of Chemotherapy-Induced Peripheral Neuropathy: A ReviewMed Sci Monit In Press; DOI: 10.12659/MSM.951283
Clinical Research
Sensory Processing, Dissociation, and Affective Symptoms in Misophonia: A Cross-Sectional Study of 35 AdultsMed Sci Monit In Press; DOI: 10.12659/MSM.950938
Most Viewed Current Articles
17 Jan 2024 : Review article 10,187,196
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,708,487
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,341,643
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 706,524
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387