17 September 2020: Clinical Research
Comparison of Clinical Outcomes in Patients with ST Elevation Myocardial Infarction with Percutaneous Coronary Intervention and the Use of a Telemedicine App Before and After the COVID-19 Pandemic at a Center in Beijing, China, from August 2019 to March 2020
Jing Nan1ABCDEG*, Shuai Meng1BCE, Hongyu Hu1CDE, Ruofei Jia1DEF, Wei Chen1DEF, Qun Li1DE, Tong Zhang1DEF, Ke Song1DEF, Yang Wang2ACDE, Zening Jin1ABCDEFDOI: 10.12659/MSM.927061
Med Sci Monit 2020; 26:e927061






Abstract
BACKGROUND: The efficacy of telemedicine in reducing delay times and short-term adverse clinical outcomes in patients with ST segment elevation myocardial infarction (STEMI) during the coronavirus disease 2019 (COVID-19) pandemic is unclear. This study compared outcomes in patients with STEMI who had percutaneous coronary intervention (PCI) and the use of a telemedicine app from August 2019 to March 2020 at a single center in Beijing, China.
MATERIAL AND METHODS: A total of 243 patients with STEMI who underwent PCI were consecutively enrolled and divided into 2 groups according to the date, before or after the pandemic. The 2 groups were further divided into patients who used the app for consulting and those who did not.
RESULTS: The time from symptom onset to calling an ambulance (SCT), door to balloon time (DTB), and total ischemia time (TIT) were significantly prolonged in patients after the pandemic. Patients who used the app had shorter SCT, DTB, and TIT before and after the pandemic compared to those who did not. Adverse clinical outcomes were significantly higher after compared with before the pandemic, despite the incidence rate of stroke, any revascularization, and stent thrombosis. However, there was no significant difference in short-term adverse clinical outcomes between patients who used the app and those who did not before and after the pandemic.
CONCLUSIONS: Telemedicine reduced the delay time of STEMI patients during the COVID-19 pandemic. The difference in short-term adverse clinical outcomes was not statistically significant between patients who used the app and those who did not.
Keywords: acute coronary syndrome, COVID-19, Telemedicine, Betacoronavirus, COVID-19, Combined Modality Therapy, Comorbidity, Coronary Angiography, Coronavirus Infections, Hospital Mortality, Mobile Applications, Pandemics, percutaneous coronary intervention, Pneumonia, Viral, SARS-CoV-2, ST elevation myocardial infarction, Smartphone, Time Factors, Time-to-Treatment
Background
Coronavirus disease 2019 (COVID-19), which is caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), is presently a global pandemic [1]. The normal performance of medical services and the willingness of patients to seek treatment are compromised [2]. Acute ST segment elevation myocardial infarction (STEMI), a type of cardiovascular emergence, causes a large number of deaths in modern society. The prevalence of STEMI may increase under the social and psychosocial pressure caused by COVID-19 [3]. The importance of reducing the total ischemia time (TIT) to as short as possible is well recognized because opportune reperfusion therapy is related with marked improvement in clinical outcomes of STEMI patients [4–7]. The potential impact of COVID-19 on pre- and post-hospital delay times and short-term adverse clinical outcomes in patients with STEMI is unclear.
Telemedicine is a useful tool to improve health care performance and has been proven to be effective for the management of STEMI patients [8–10]. The crucial role of telemedicine in medical services during the COVID-19 pandemic has been discussed in several review articles [11–13]. However, the efficacy of telemedicine in reducing delay times and short-term adverse clinical outcomes in STEMI patients undergoing primary percutaneous coronary intervention (PCI) during the COVID-19 pandemic is ill-defined. In August 2019, our center developed a free-of-charge application (the Tiantanzhixin app) that enabled online communication between patients and doctors to improve the management quality of patients with chronic diseases. As of March 31, 2020, 4 866 patients had downloaded this app. Some app users developed STEMI and consulted online via the app before and after the COVID-19 pandemic.
This study aimed to compare the clinical outcomes in patients with STEMI and PCI who used the telemedicine app with those patients who did not use the app before and after the COVID-19 pandemic from August 2019 to March 2020 at a single center in Beijing, China.
Material and Methods
STUDY DESIGN AND PARTICIPANTS:
This was a single-center observational study conducted at the Beijing Tiantan Hospital, Capital Medical University, a large tertiary hospital in Beijing, China. Patients diagnosed with acute STEMI who underwent primary PCI within 24 h after symptom onset at our center from August 1, 2019, to March 31, 2020, were consecutively enrolled. STEMI was diagnosed according to the universal definition: myocardial ischemia symptoms with ST segment elevation >2 mm in V2–V3 or >1 mm in other contiguous leads, or a new left bundle branch block. Patients were excluded from the study for the following reasons: patient refused or did not undergo primary PCI; patients with STEMI due to stent thrombosis; and patients with mechanical complications. The study flowchart is shown in the Figure 1.
Demographic characteristics, comorbidities, and risk factors including hypertension, dyslipidemia, diabetes mellitus, and smoking were collected and analyzed. Clinical manifestation (Killip classification, hypotension, or cardiac shock) and risk stratification of the enrolled patients were documented and analyzed. Cardiogenic shock was diagnosed when the systolic blood pressure of STEMI patients was <90 mmHg or ≥90 mmHg with the need of therapeutically or mechanical support combined with hypoperfusion signs and a heart rate of ≥60 beats/min. Risk stratification was scored by the Global Registry of Acute Coronary Events (GRACE) scoring system which has 8 clinical variables ranging from 2 to 372 and the Thrombolysis in Myocardial Infarction (TIMI) scoring system which has 7 clinical variables ranging from 0 to 7 [14,15]. The coronary anatomy severity was scored using the Synergy Between Percutaneous Coronary Intervention with Taxus and Cardiac Surgery (Syntax) score [16]. Upon admission, laboratory test results, including peak cardiac troponin I during hospitalization, B-type natriuretic peptide (BNP), and left ventricular ejection fraction, were also collected.
STUDY ENDPOINTS:
The critical time intervals, namely, the time from symptom onset to calling ambulance (SCT), calling ambulance to first medical contact (FMC) arrival time, FMC to hospital arrival time, door to balloon (DTB) time, and TIT were retrieved. Short-term adverse clinical outcomes were also documented and compared. The adverse clinical outcomes included major adverse cardiac event (MACE), all-causes of death, cardiac death, non-fatal myocardial infarction, stroke, any revascularization, definite or probable stent thrombosis, and new renal replacement therapy. MACE was defined as the composite of death, myocardial infarction, and any revascularization. Cardiac death was diagnosed as any death due to cardiac or procedure-related causes. All of the deaths were considered cardiac related unless an unequivocal non-cardiac cause could be established. Myocardial infarction was defined by the following parameters: presence of clinical symptoms, electrocardiogram (ECG) changes or abnormal imaging findings indicative of myocardial infarction, and an increase in creatine kinase myocardial band fraction above the upper normal limits or an increase in troponin I above the 99th percentile. Stroke was diagnosed with the presence of a new focal neurological deficit with signs or symptoms persisting for 24 h and in the presence of cerebral lesions, which were detected by imaging procedures. Any revascularization was defined as a second PCI or coronary bypass surgery in the target vessel. Stent thrombosis was classified using the Academic Research Consortium definition [17]. In-hospital adverse events were recorded from patient electronic medical records, and 30-day adverse events were evaluated by telephone interviews, outpatient visits, or through the Tiantanzhixin app.
SCREENING PROTOCOL OF STEMI PATIENTS AT BEIJING TIANTAN HOSPITAL DURING THE COVID-19 PANDEMIC:
During the pandemic, there was no restriction on the normal movements of patients; however, there were strict screening protocols to reduce the risk of cross infection. In our hospital, all of the STEMI patients who intended to undergo primary PCI received COVID-19 screening before starting the primary PCI procedure after January 31, 2020, the day Wuhan was locked down. The screening protocol was as follows at our center: If a patient had fever or suspicious medical contact history in Hubei province, thrombolytic therapy was recommended instead of primary PCI. If a patient had no signs of infection and no suspicious medical contact history, he or she underwent primary PCI if the screening examination, including the complete blood count and chest computed tomography (CT), was normal. If a patient had no signs of infection and no suspicious medical history but the complete blood count or chest CT were suspicious for COVID-19 infection, he or she did not undergo primary PCI until a throat swab nucleic acid test was negative. The nucleic acid test was examined by reverse transcription polymerase chain reaction (RT-PCR) assays. RT-PCR was conducted with primers and probes targeting the ORF1ab and N genes and a positive reference gene according to the manufacturer’s specifications (Beijing Yocon Biology Co Ltd., China). The diagnosis and management of patients with COVID-19 was conducted according to the current clinical guideline [18]. None of the patients enrolled in our study were diagnosed with COVID-19.
DETAILED INFORMATION ON THE TIANTANZHIXIN APPLICATION:
The Tiantanzhixin app is a free-of-charge application designated for smart phones. All of the patients who visited the outpatient clinic or chest pain center, or were hospitalized in our department for any reason were recommended to install this app by scanning a quick response code. This novel application has bilateral communication functions that support real-time home-to-hospital interactions and online consulting. All of the patients who successfully installed the app can communicate with doctors online anytime using voice messages, text messages, or pictures. Trained professionals answer the patients’ questions.
PRIMARY PCI PROCEDURE AND OPTIMAL MEDICAL THERAPY:
Primary PCI was performed by trained clinicians using the standard technique via radial or femoral access routes, according to the recommendations from current guidelines. The employ of thrombus aspiration catheter, intra-aortic balloon counter-pulsation (IABP), temporary pacemaker, lesion preparation, stent implantation, post-dilation, and the use of glycoprotein IIb/IIIa inhibitor (GPI) and anticoagulation regimens were left to the discretion of the clinician. All of the patients were prescribed aspirin (600 mg for loading dose, 100 mg per day for maintenance) in combination with clopidogrel (600 mg for loading dose, 75 mg per day for maintenance) or ticagrelor (180 mg for loading dose, 90 mg twice per day for maintenance). Angiotensin-converting enzyme (ACE) inhibitors, angiotensin receptor blockers (ARB), β blockers, statins, and other medical therapies were prescribed as the guidelines recommended.
All of the patients provided written informed consent. Ethical approval was granted by the Beijing Tiantan Hospital, Capital Medical University.
STATISTICAL ANALYSIS:
Categorical variables were expressed as total numbers and percentages and were compared between groups by the chi-squared test and Yate’s continuity correction when the total counts per category <5. Continuous variables were expressed as mean±SD or median (quartiles 1 and 3) and compared using the independent sample
Results
COMPARISON OF BASELINE CLINICAL CHARACTERISTICS:
The comparison of baseline clinical characteristics between the app user group and non-app user group before and after the pandemic are presented in Table 1. The differences between the patients before or after the pandemic regarding age, sex, and common comorbidities were not statistically significant, except that the incidence rate of hypertension and previous cerebrovascular events were lower in the patients after the pandemic compared with the patients before the pandemic (40.00% vs. 63.39%, P=0.002; 10.00% vs. 25.68%, P=0.011, respectively). The baseline medication therapy, BNP on admission, and left ventricular ejection fraction were comparable between the 2 groups. The peak cardiac troponin I level was higher in the patients after the pandemic compared with those before the pandemic, but the difference was not statistically significant (100.98±35.16 vs. 91.51±26.98, P=0.06, respectively). The patients after the pandemic had a higher possibility of having Killip classification ≥2 than did patients before the pandemic (60.00% vs. 40.40%, P=0.011). Before the pandemic, the patients who used the app had lower rates of hypertension than the patients who did not use the app (32.00% vs. 68.40%, P=0.001), while the rate of prior percutaneous coronary intervention was higher in the patients who used the app, although the difference was not statistically significant (28.00% vs. 12.00%, P=0.058).
COMPARISON OF ANGIOGRAPHIC AND PRIMARY PCI PROCEDURAL CHARACTERISTICS:
The comparison of coronary angiographic and primary PCI procedural characteristics between the app user group and non-app user group before and after the pandemic are presented in Table 2. There were no significant differences in the pre-procedure TIMI flow grade, severity of coronary artery disease, location of infarct-related artery, and usage of temporary pacemakers between the patients before and after the pandemic. However, the patients after the pandemic had lower levels of post-procedure TIMI flow compared to those before the pandemic (3 [2–3] vs. 3 [3–3], P=0.000), higher rates of anterior wall infarction (68.33% vs. 54.64%, P=0.045), higher rates of IABP usage (35.00% vs. 16.40%, P=0.003) and vasopressor usage (58.30% vs. 40.40%, P=0.017), and higher GRACE scores (172.25±20.38 vs. 165.92±19.75, P=0.034). The angiographic and primary PCI procedural characteristics were comparable between the patients who used the app and the patients who did not.
COMPARISON OF THE CRITICAL TIME INTERVAL:
The critical time intervals between the app user group and non-app user group before and after the pandemic are presented in Table 3. The SCT, DTB, and TIT were significantly prolonged in the patients after the pandemic compared with those before the pandemic (68 [56.5–90] min vs. 60 [47–78] min, P=0.023; 76.5 [65.25–85] min vs. 50 [40–60] min, P=0.000; and 185 [165.25–210.25] min vs. 150 [131–174] min, P=0.000, respectively). However, the SCT to the FMC arrival and the time from FMC to hospital arrival time were comparable between patients before and patients after the pandemic (20 [16–23.75] min vs. 20 [16–24], P=0.900; 17 [14–21] min vs. 18 [15–22] min, P=0.06, respectively). Compared with the patients who did not use the app, those who used the app had shorter SCT, DTB, and TIT before (61 [9.75–80] min vs. 45 [40–60] min, P=0.000; 45 [33–50] min vs. 50 [42.75–64.25] min, P=0.002; and 128 [116–142.5] min vs. 157 [135.5–177] min, P=0.000, respectively) and after the pandemic (47.5 [45–60] min vs. 70 [60–90] min, P=0.007; 65 [56.25–73.5] min vs. 77 [70–86.5] min, P=0.010; and 144.5 [132.75–162.5] min vs. 188 [171–213] min, P=0.001, respectively).
COMPARISON OF IN-HOSPITAL AND 30-DAY ADVERSE CLINICAL OUTCOME:
The incidence rate of both in-hospital and 30-day adverse clinical outcomes between the app user group and non-app user group are presented in Table 4. The in-hospital and 30-day follow-up adverse clinical outcomes, including all-cause mortality, cardiac death, MACE, non-fatal myocardial infarction, and new renal replacement therapy, were significantly higher in patients after the pandemic than in those before the pandemic, while stroke, any revascularization, and stent thrombosis were comparable between the 2 groups. However, the incidence rates of in-hospital and 30-day follow-up adverse clinical outcomes were comparable between the app user group and non-app user group before and after the pandemic.
Discussion
In this single-center retrospective observational study, the delay times in the STEMI patients after the pandemic were significantly prolonged compared to those before the pandemic. The prolonged pre- and post-hospital delay times further translated into higher rates of short-term adverse clinical outcomes. Telemedicine (via the Tiantanzhixin app) was effective for reducing delay times before and after the pandemic, but there was no significant difference in the incidence rates of short-term adverse clinical outcomes between the app user group and non-app user group before and after the pandemic in our study.
Primary PCI is recommended as the first-line therapy for treating acute STEMI patients [5–7]. But this recommendation is based on the normal performance of health care services. Thrombolytic therapy is considered the first-line therapy during the COVID-19 pandemic, according to the expert consensus of the Chinese Society of Cardiology, to decrease the risk of cross infection [19]. Based on experiences in China and other countries, the use of proper personal protective equipment (PPE) should be considered for persons performing primary PCI [20–24]. However, a reduction in patients who underwent primary PCI was observed, which was associated with a concern of cross infection from both doctors and patients [25–27]. The number of STEMI patients who underwent primary PCI in this center did not decrease during the pandemic, which could be explained by the following: First and foremost, Beijing Tiantan Hospital was one of the few hospitals in Beijing where primary PCI was still available when other hospitals decided to shut down primary PCI during the COVID-19 pandemic, so additional patients might have been transferred to our center. Second, the risk of cross infection was relatively low in Beijing during the pandemic as compared with other countries.
The critical role of telemedicine during the COVID-19 pandemic was discussed in several articles that mentioned the potential benefit and inherent issues in telemedicine [11–13,28–31]. However, unlike our study, all of these articles proposed the importance of telemedicine during the pandemic but lacked specific clinical information to support their ideas.
This study produced some important findings. The first is that the delay times (both pre- and post-hospital) of STEMI patients were prolonged after the COVID-19 pandemic compared with the delay times before the pandemic. The increased pre-hospital delays were mostly related to the SCT, while the SCT to FMC arrival time and the FMC to hospital arrival time did not increase. Traditional pre-hospital delays include patient delays and emergency services delays [32,33]. In the present study, pre-hospital delays, including the SCT to the FMC and the FMC to hospital arrival time, were not influenced by COVID-19. The patient delays, judging from our results, were mostly related to increased pre-hospital delays during the pandemic. The reasons for the prolonged patient delays were associated not only with public awareness of how to recognize common acute myocardial infarction symptoms and call emergency services, but also with the fear of cross infection during the pandemic [2,3,5]. The prolonged post-hospital delay times were largely related to the screening protocol when medical quarantine was needed. In order to reduce the risk of cross infection, health care facilities established strict screening protocols to identify COVID-19 patients, which led to the deterioration of patients with STEMI by prolonging the delay times, even after the patients arrived at the hospital. This is consistent with the latest findings from Hong Kong in which increased delay times, especially prolonged waiting times after arrival for patients with STEMI, were observed [34].
The second finding of the present study is the usefulness of telemedicine at reducing pre- and post-hospital delay times during the pandemic. Telemedicine has been demonstrated to be effective at reducing delay times in patients with STEMI [35–38], but all of the conclusions made by these studies were based on the normal functioning of health care facilities, when there were no screening protocols in place. To our knowledge, the present study is the first to explore the efficacy of telemedicine for reducing delay times in patients with STEMI during the COVID-19 pandemic. After comparing the critical time intervals of the app user group and non-app user group before and after the pandemic, we found that the patients in the app user group had shorter pre- and post-hospital delay times. The significant reduction in the pre- and post-hospital delay times in the app user group was related to the diminished fear of cross infection among the STEMI patients and better preparation after their arrival to reduce waiting and screening protocol times.
This study’s third finding is the significantly increased rates of both in-hospital and 30-day adverse clinical outcomes after the pandemic. There are many reasons which could explained this. First, the prolonged delay times increased the total ischemia times, which may have further compromised hemodynamic stability and influenced clinical outcomes [39]. Several patients died during the screening protocols before they could undergo primary PCI at our center. Second, the proportion of patients with anterior wall myocardial infarction increased after the pandemic with an elevated proportion of cardiogenic shock, no-flow phenomena, and IABP usage. Lastly, a higher risk of STEMI patients with higher GRACE scores was another potential reason.
This study’s final finding was that the rates of short-term adverse clinical outcomes were comparable between the patients who used the app for telemedicine support and those who did not. Although studies have demonstrated the efficacy of telemedicine for reducing short-term adverse clinical outcomes in patients with STEMI [40,41], there was no significant change in the incidence rate of in-hospital and 30-day follow-up adverse clinical outcomes in the present study. The reduction in TIT did not translate into clinical benefits for the app user group because of the limited number of patients who participated and the shorter follow-up periods with relatively low incidence rates of adverse clinical outcomes.
COVID-19 has had an obviously negative impact on the management of STEMI patient care, including prolonged delay times, which may further influence these patients’ clinical outcomes. Timely reperfusion therapy with reduced TIT is the key principle for the management of patients with STEMI, which is more complicated than ever before in the context of the COVID-19 pandemic. The results of our study demonstrate the efficacy of telemedicine at reducing delay times in STEMI patients, similar to other studies. However, our study is the first to prove the efficacy of telemedicine use in patients with STEMI during the COVID-19 pandemic. Properly managing the care of patients with STEMI by reducing delay times as much as possible and lessening the adverse impact of COVID-19 is critical and challenging during the pandemic while the number of new COVID-19 cases increases globally and social distancing and quarantines are deemed necessary [42].
Conclusions
This study demonstrated the efficacy of telemedicine for the management of patients with STEMI during the COVID-19 pandemic. In conclusion, COVID-19 prolonged pre- and post-hospital delay times in STEMI patients. Telemedicine appears to be useful by reducing delay times during the COVID-19 pandemic, although there was no statistical difference in short-term adverse clinical outcomes between the patients who used telemedicine and those who did not.
Several limitations should be considered when interpreting this study. First, this is an observational study so potential confounding factors and biases may be present. Second, our study had a relatively small number of participants and a short-term follow-up period. Third, the severity of COVID-19 cross infection risk and PPE supplies vary in different regions and, therefore, this study’s conclusions are limited to circumstances in which the risk of cross infection is relatively low and PPE supplies are sufficient.
Further research is necessary. Prospective multi-center studies with more participants and longer follow-up periods are needed to verify our conclusions. Also, different age groups and regions with different cross infection risk levels should be included in future research. Also, whether this study’s conclusions can be extended to the management of other cardiovascular emergencies remains unclear.
Figures
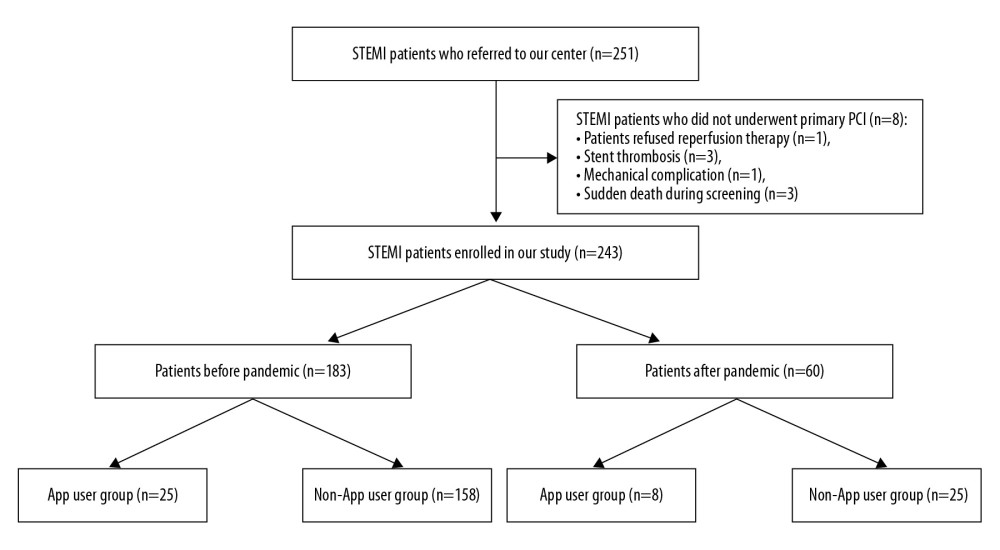 Figure 1. Study flowchart.
Figure 1. Study flowchart. Tables
Table 1. Baseline clinical characteristics of the app user group and non-app user group before and after the COVID-19 pandemic.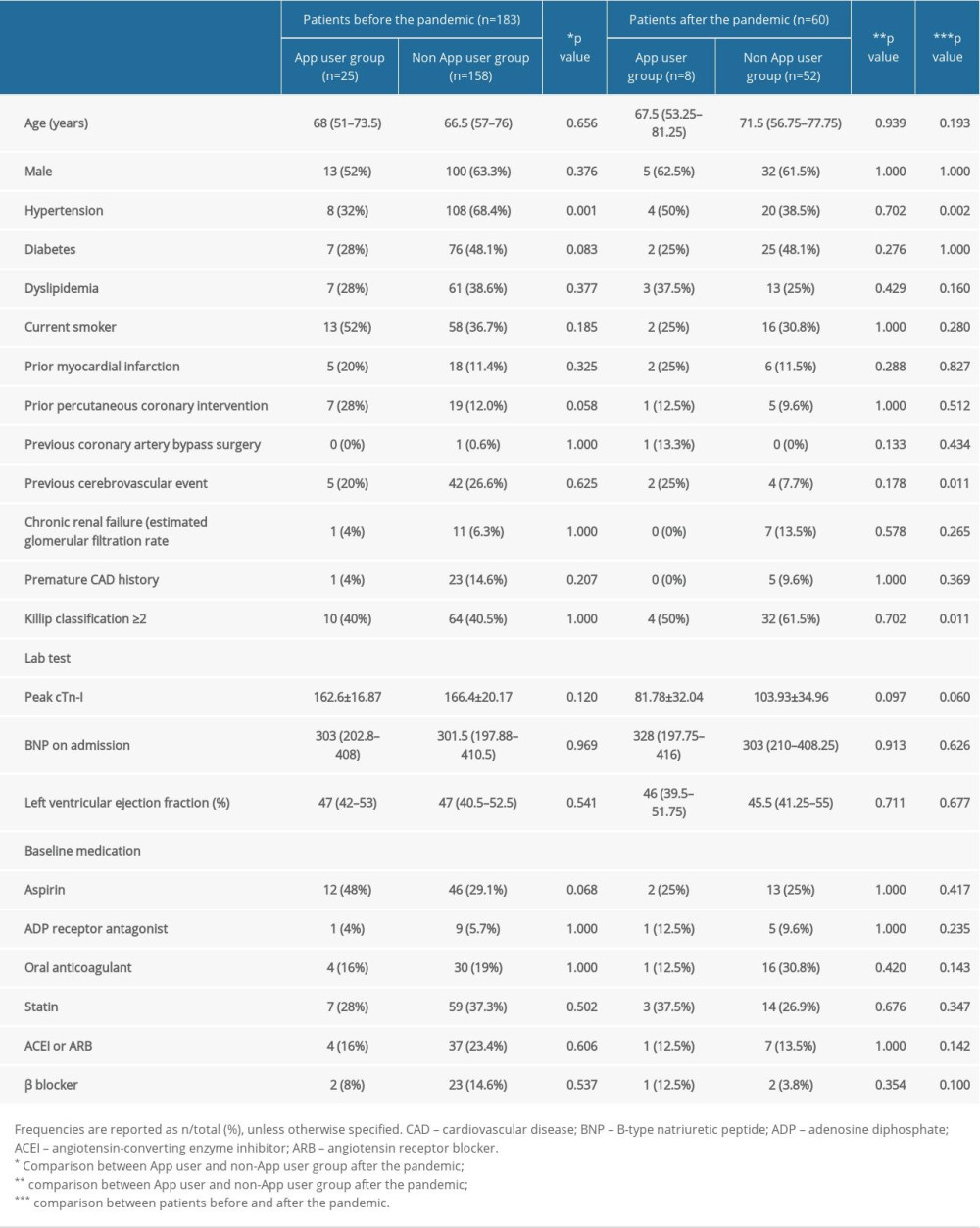 Table 2. Baseline angiographic and primary percutaneous coronary intervention (primary PCI) of the app user group and non-app user group before and after the COVID-19 pandemic.
Table 2. Baseline angiographic and primary percutaneous coronary intervention (primary PCI) of the app user group and non-app user group before and after the COVID-19 pandemic.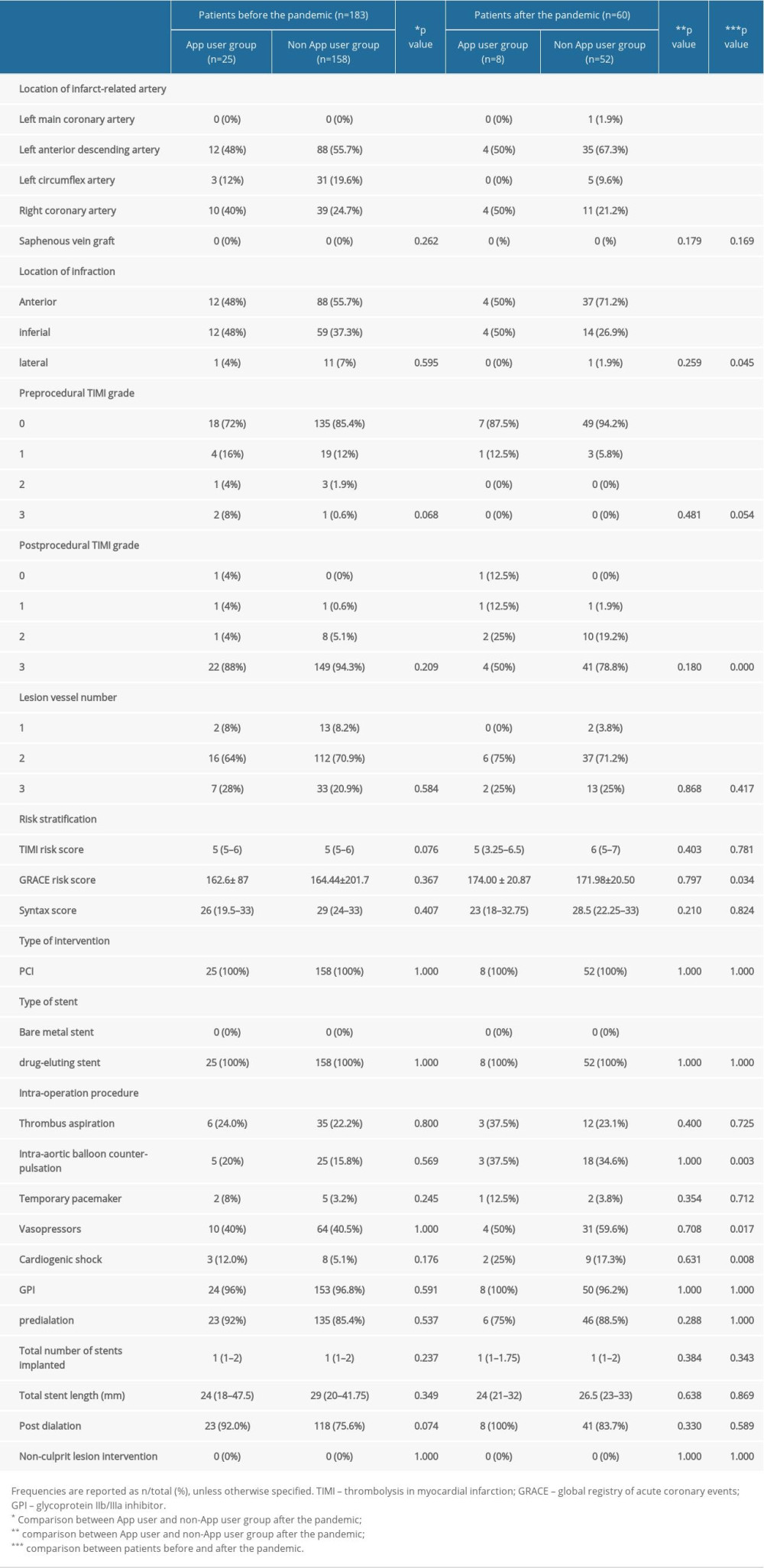 Table 3. Comparison of the critical time intervals between the app user group and non-app user group before and after the COVID-19 pandemic.
Table 3. Comparison of the critical time intervals between the app user group and non-app user group before and after the COVID-19 pandemic.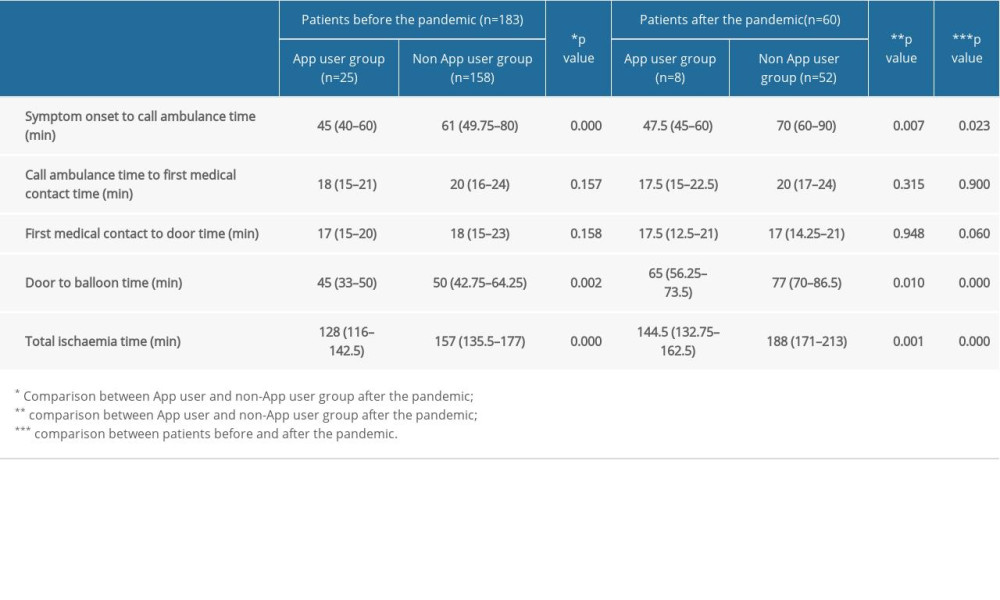 Table 4. Comparison of the incidence of adverse events between the app user group and non-app user group before and after the COVID-19 pandemic.
Table 4. Comparison of the incidence of adverse events between the app user group and non-app user group before and after the COVID-19 pandemic.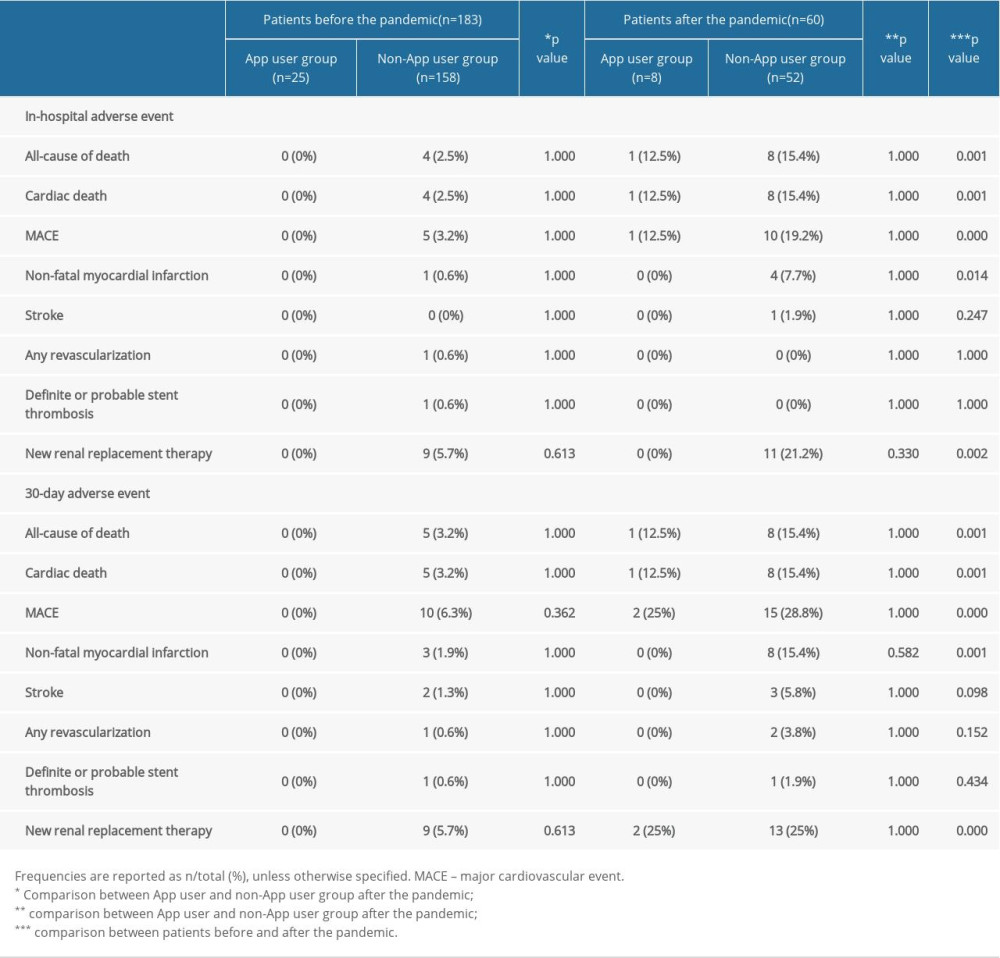
References
1. Cucinotta D, Vanelli M, WHO declares COVID-19 a pandemic: Acta Biomed, 2020; 91; 157-60
2. Masroor S, Collateral damage of COVID-19 pandemic: Delayed medical care: J Card Surg, 2020; 35; 1345-47
3. Roffi M, Guagliumi G, Ibanez B, The obstacle course of reperfusion for STEMI in the COVID-19 pandemics: Circulation, 2020; 141; 1951-53
4. Scholz KH, Maier SKG, Maier LS, Impact of treatment delay on mortality in ST-segment elevation myocardial infarction (STEMI) patients presenting with and without haemodynamic instability: Results from the German prospective, multicentre FITT-STEMI trial: Eur Heart J, 2018; 39; 1065-74
5. Ibanez B, James S, Agewall S, 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC): Eur Heart J, 2018; 39; 119-77
6. O’Gara PT, Kushner FG, Ascheim DD, 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines [published correction appears in Circulation, 2013; 128(25): e481]: Circulation, 2013; 127(4); e362-425
7. Levine GN, Bates ER, Blankenship JC, 2015 ACC/AHA/SCAI Focused Update on Primary Percutaneous Coronary Intervention for Patients With ST-Elevation Myocardial Infarction: An Update of the 2011 ACCF/AHA/SCAI Guideline for Percutaneous Coronary Intervention and the 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction [published correction appears in J Am Coll Cardiol, 2016; 67(12): 1506]: J Am Coll Cardiol, 2016; 67(10); 1235-50
8. Rasmussen MB, Frost L, Stengaard C, Diagnostic performance and system delay using telemedicine for prehospital diagnosis in triaging and treatment of STEMI: Heart, 2014; 100; 711-15
9. Brunetti ND, De Gennaro L, Correale M, Pre-hospital electrocardiogram triage with telemedicine near halves time to treatment in STEMI: A meta-analysis and meta-regression analysis of non-randomized studies: Int J Cardiol, 2017; 232; 5-11
10. Mehta S, Botelho R, Cade J, Global challenges and solutions: Role of telemedicine in ST-elevation myocardial infarction interventions: Interv Cardiol Clin, 2016; 5; 569-81
11. Bokolo AJ, Use of Telemedicine and Virtual Care for Remote Treatment in Response to COVID-19 Pandemic: J Med Syst, 2020; 44; 132
12. Vidal-Alaball J, Acosta-Roja R, Pastor Hernández N, Telemedicine in the face of the COVID-19 pandemic: Aten Primaria, 2020; 52(6); 418-22
13. Bokolo AJ, Exploring the adoption of telemedicine and virtual software for care of outpatients during and after COVID-19 pandemic: Ir J Med Sci, 2020 [Online ahead of print]
14. Lev EI, Kornowski R, Vaknin-Assa H, Comparison of the predictive value of four different risk scores for outcomes of patients with ST-elevation acute myocardial infarction undergoing primary percutaneous coronary intervention: Am J Cardiol, 2008; 102(1); 6-11
15. Duman H, Çetin M, Durakoğlugil ME, Relation of angiographic thrombus burden with severity of coronary artery disease in patients with ST segment elevation myocardial infarction: Med Sci Monit, 2015; 21; 3540-46
16. van Dongen IM, Elias J, García-García HM, Value of the SYNTAX score in ST-elevation myocardial infarction patients with a concomitant chronic total coronary occlusion (from the EXPLORE Trial): Am J Cardiol, 2019; 123(7); 1035-43
17. Applegate RJ, Sacrinty MT, Little WC, Incidence of coronary stent thrombosis based on academic research consortium definitions: Am J Cardiol, 2008; 102(6); 683-88
18. Jin YH, Cai L, Cheng ZS, A rapid advice guideline for the diagnosis and treatment of 2019 novel coronavirus (2019-nCoV) infected pneumonia (standard version): Mil Med Res, 2020; 7(1); 4
19. Han Y, Zeng H, Jiang H, CSC expert consensus on principles of clinical management of patients with severe emergent cardiovascular diseases during the COVID-19 epidemic: Circulation, 2020; 141; e810-16
20. Abdi S, Salarifar M, Mortazavi SH, COVID-19 sends STEMI to quarantine!?: Clin Res Cardiol, 2020 [Online ahead of print]
21. Kirtane AJ, Bangalore S, Why fibrinolytic therapy for ST-segment-elevation myocardial infarction in the COVID-19 pandemic is not your new best friend: Circ Cardiovasc Qual Outcomes, 2020; 13; e006885
22. Mahmud E, Dauerman HL, Welt FGP, Management of acute myocardial infarction during the COVID-19 pandemic: A Consensus Statement from the Society for Cardiovascular Angiography and Interventions (SCAI), the American College of Cardiology (ACC), and the American College of Emergency Physicians (ACEP): Catheter Cardiovasc Interv, 2020; 96(2); 336-45
23. Stefanini GG, Montorfano M, Trabattoni D, ST-elevation myocardial infarction in patients with COVID-19: Clinical and angiographic outcomes: Circulation, 2020; 141; 2113-16
24. Zeng J, Huang J, Pan L, How to balance acute myocardial infarction and COVID-19: The protocols from Sichuan Provincial People’s Hospital: Intensive Care Med, 2020; 46; 1-3
25. De Rosa S, Spaccarotella C, Basso C, Reduction of hospitalizations for myocardial infarction in Italy in the COVID-19 era: Eur Heart J, 2020; 41; 2083-88
26. Hammad TA, Parikh M, Tashtish N, Impact of COVID-19 pandemic on ST-elevation myocardial infarction in a non-COVID-19 epicenter: Catheter Cardiovasc Interv, 2020 [Online ahead of print]
27. Garcia S, Albaghdadi MS, Meraj PM, Reduction in ST-segment elevation cardiac catheterization laboratory activations in the United States during COVID-19 pandemic: J Am Coll Cardiol, 2020; 75; 2871-72
28. Hollander JE, Carr BG, Virtually perfect? Telemedicine for Covid-19: N Engl J Med, 2020; 382(18); 1679-81
29. Nørgaard K, Telemedicine consultations and diabetes technology during COVID-19: J Diabetes Sci Technol, 2020; 14(4); 767-68
30. Iyengar K, Jain VK, Vaishya R, Pitfalls in telemedicine consultations in the era of COVID 19 and how to avoid them [published online ahead of print, 2020 Jun 9]: Diabetes Metab Syndr, 2020; 14(5); 797-99
31. Mahajan V, Singh T, Azad C, Using telemedicine during the COVID-19 pandemic: Indian Pediatr, 2020; 57(7); 652-57
32. Gadella A, Sastre MÁ, Maicas C, ST-segment elevation myocardial infarction in times of COVID-19: Back to the last century? A call for attention: Rev Esp Cardiol (Engl Ed), 2020; 73(7); 582-83
33. Wang TY, Nallamothu BK, Krumholz HM, Association of door-in to door-out time with reperfusion delays and outcomes among patients transferred for primary percutaneous coronary intervention: JAMA, 2011; 305; 2540-47
34. Tam CF, Cheung KS, Lam S, Impact of coronavirus disease 2019 (COVID-19) outbreak on ST-segment-elevation myocardial infarction care in Hong Kong, China: Circ Cardiovasc Qual Outcomes, 2020; 13(4); e006631
35. Brunetti ND, De Gennaro L, Correale M, Pre-hospital electrocardiogram triage with telemedicine near halves time to treatment in STEMI: A meta-analysis and meta-regression analysis of non-randomized studies: Int J Cardiol, 2017; 232; 5-11
36. Caldarola P, Gulizia MM, Gabrielli D, ANMCO/SIT Consensus Document: telemedicine for cardiovascular emergency networks: Eur Heart J Suppl, 2017; 19(Suppl D); D229-43
37. Goebel M, Bledsoe J, Push notifications reduce Emergency Department response times to prehospital ST-segment elevation myocardial infarction: West J Emerg Med, 2019; 20(2); 212-18
38. Brunetti ND, Dell’Anno A, Martone A, Prehospital ECG transmission results in shorter door-to-wire time for STEMI patients in a remote mountainous region: Am J Emerg Med, 2020; 38; 252-57
39. Foo CY, Bonsu KO, Nallamothu BK, Coronary intervention door-to-balloon time and outcomes in ST-elevation myocardial infarction: A meta-analysis: Heart, 2018; 104(16); 1362-69
40. Sakai T, Nishiyama O, Onodera M, Predictive ability and efficacy for shortening door-to-balloon time of a new prehospital electrocardiogram-transmission flow chart in patients with ST-elevation myocardial infarction-Results of the CASSIOPEIA study: J Cardiol, 2018; 72(4); 335-42
41. Sanchez-Ross M, Oghlakian G, Maher J, The STAT-MI (ST-segment analysis using wireless technology in acute myocardial infarction) trial improves outcomes: JACC Cardiovasc Interv, 2011; 4; 222-27
42. Yerasi C, Case BC, Forrestal BJ, Treatment of ST-segment elevation myocardial infarction during COVID-19 pandemic: Cardiovasc Revasc Med, 2020 [Online ahead of print]
Figures
Tables
Table 1. Baseline clinical characteristics of the app user group and non-app user group before and after the COVID-19 pandemic.Table 2. Baseline angiographic and primary percutaneous coronary intervention (primary PCI) of the app user group and non-app user group before and after the COVID-19 pandemic.Table 3. Comparison of the critical time intervals between the app user group and non-app user group before and after the COVID-19 pandemic.Table 4. Comparison of the incidence of adverse events between the app user group and non-app user group before and after the COVID-19 pandemic.Table 1. Baseline clinical characteristics of the app user group and non-app user group before and after the COVID-19 pandemic.Table 2. Baseline angiographic and primary percutaneous coronary intervention (primary PCI) of the app user group and non-app user group before and after the COVID-19 pandemic.Table 3. Comparison of the critical time intervals between the app user group and non-app user group before and after the COVID-19 pandemic.Table 4. Comparison of the incidence of adverse events between the app user group and non-app user group before and after the COVID-19 pandemic. In Press
Clinical Research
Institutional and Regional Variations in Access to Clinical Trials and Next-Generation Sequencing in Turkis...Med Sci Monit In Press; DOI: 10.12659/MSM.951027
Clinical Research
Low-Intensity Blood Flow-Restricted Multi-Joint Exercise Improves Muscle Function in Patients With Patellof...Med Sci Monit In Press; DOI: 10.12659/MSM.950516
Review article
Musculoskeletal Ultrasound and MRI in the Evaluation of Chemotherapy-Induced Peripheral Neuropathy: A ReviewMed Sci Monit In Press; DOI: 10.12659/MSM.951283
Clinical Research
Sensory Processing, Dissociation, and Affective Symptoms in Misophonia: A Cross-Sectional Study of 35 AdultsMed Sci Monit In Press; DOI: 10.12659/MSM.950938
Most Viewed Current Articles
17 Jan 2024 : Review article 10,187,196
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,708,487
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,341,643
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 706,524
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387