02 November 2020: Clinical Research
The Reliability of MyotonPRO in Assessing Masseter Muscle Stiffness and the Effect of Muscle Contraction
Jia-feng Yu1BDEF, Tian-tian Chang2BDEF, Zhi-jie Zhang3AC*DOI: 10.12659/MSM.926578
Med Sci Monit 2020; 26:e926578






Abstract
BACKGROUND: Temporomandibular disorders (TMD) are accompanied by masticatory muscle-related pain, making it meaningful to assess the stiffness of the masticatory muscles. The present study investigated the intra- and inter-operator reliabilities of MyotonPRO for assessing the elasticity of masseter muscles, to determine minimal detectable changes, and to quantify changes in stiffness from conditions of relaxation to maximal contraction.
MATERIAL AND METHODS: Twenty healthy subjects (10 men and 10 women) were recruited. The stiffness of their masseter muscles was quantified with MyotonPRO in both relaxed and maximal contraction conditions. Two experienced operators (A and B) measured stiffness on the same day, and operator A repeated this procedure 5 days later.
RESULTS: Intra-rater reliability was good (ICC=0.78) and inter-operator reliability was excellent (ICC=0.95) for assessing masseter muscle stiffness with MyotonPRO. The mean stiffness of the masseter muscle on the dominant side was 369.5 N/m under relaxed conditions and 618.3 N/m at maximum bite force, an increase of 67.4%. Stiffness on the dominant and non-dominant sides did not differ significantly under both conditions (P>0.05).
CONCLUSIONS: MyotonPRO is a reliable method for quantifying the stiffness of the masseter muscle and monitoring its changes under different contraction conditions.
Keywords: Elasticity, Isometric Contraction, Masseter Muscle, Reproducibility of Results, Bite Force, Electromyography, Muscle Contraction, Observer Variation
Background
Temporomandibular disorders (TMD) are common conditions, characterized by pain symptoms and associated with abnormalities in the masticatory muscles and temporomandibular joint (TMJ) [1]. Although 60% to 70% of the normal population have been reported to experience TMD, only around 15% are conscious of their TMD symptoms [1,2]. As a primary cause of masticatory dysfunction, TMD affects activities of daily life and, in particular, leads to psychological problems [3,4]. Efforts to prevent or ameliorate TMD may therefore improve patient quality of life.
Masticatory muscles play an important role in maintaining a balance in masticatory function. Moreover, bite forces influence the masticatory muscles to improve chewing functions [5]. Among these masticatory muscles are the masseter muscles, which help stabilize the grinding path during chewing [6], suggesting that bite forces may be associated with the masseter muscles during mastication. To our knowledge, no study to date has quantified changes in masseter muscle stiffness from conditions of relaxation to maximum bite force. Understanding of TMD may be improved by analyzing changes in the biomechanical properties of the masseter muscles in response to different conditions. Masticatory patterns differ in subjects with and without TMD, in that subjects with TMD frequently adopt a chronic unilateral chewing pattern [7]. Because equal bilateral use of the masticatory muscles during chewing can maintain the balance of masticatory function, one of the objectives of the present study was to quantify whether the biomechanical properties of masseter muscles differ on the 2 sides.
TMD is frequently accompanied by masticatory muscle pain [8], which is frequently diagnosed subjectively by physician palpation. Palpation, however, cannot assess modulations in the biomechanical properties of masseter muscles. The biomechanical properties of these muscles can be quantified by assessing fatigue, by surface electromyography (EMG), and by MyotonPRO measurements of muscle stiffness. Although alterations in masseter muscles have been evaluated by EMG [9,10], this method has limitations, as the electrical signal is easily affected by the experimental environment [11]. MyotonPRO is a convenient, portable device to quantify muscles stiffness, which can overcome the limitations of EMG. In previous studies, we used MyotonPRO to quantify the biomechanical properties of skeletal muscles, including the gastrocnemius [12] and upper trapezius [13] muscles. More importantly, we found that the stiffness of the gastrocnemius muscle and the Achilles tendon, as measured by MyotonPRO, correlated significantly with the shear modulus as quantified by shear wave elastography (SWE) [14]. These findings suggested that the MyotonPRO can quantify the stiffness of the masseter muscles under conditions of relaxation and maximal contraction, as well as the difference between them.
The aims of this investigation were to (1) determine the intra- and inter-operator reliabilities of quantifying masseter muscle stiffness and determine minimal detectable change; (2) quantify the change in stiffness from a relaxed state to maximum bite force; and (3) determine the difference in masseter muscle stiffness on both sides.
Material and Methods
ETHICS:
The study protocol was approved by the Human Subject Ethics Committee of the Luoyang Orthopedic Hospital of Henan Province (KY 2019-001-01) and conformed to the principles of the Declaration of Helsinki. Each subject provided written informed consent before the tests and was informed of all experimental procedures.
PARTICIPANTS:
Twenty healthy participants, 10 men and 10 women, with no history of TMD were recruited. Based on 3 repeated measurements in each subject, an α=0.05, an 80% power, P0 (ICC)=0.5, and P1 (ICC)=0.8, the minimal sample size for reliability analysis was calculated to be 14.4 subjects [15], indicating that 20 subjects were sufficient for reliability analyses. The demographic characteristics of all study subjects, including age, height, weight, and body mass index (BMI), were recorded.
EQUIPMENT:
MyotonPRO (Muomeetria Ltd., Tallinn, Estonia) is a hand-held device used to quantify muscle stiffness. This device operates by generating a mechanical impulse on the skin overlying the muscle being assessed, followed by MyotonPRO measurements of the mechanical oscillations of muscles produced by the mechanical impulse [16]. Muscle stiffness was measured as newtons/meter (N/m). This method can determine the resistance of the muscle to deforming forces or muscle stiffness.
PROCEDURES:
All participants were examined in the department of physiotherapy, in which the temperature was maintained around 25°C. Each subject sat on a chair and was allowed to rest for 5 minutes with their heads held in a natural position. The examination sites were marked at the highest site of the masseter muscle during jaw-clenching with maximum force. Stiffness of both sides of the masseter muscles was quantified by MyotonPRO in both relaxed and maximum bite force conditions. All measurements were taken 3 times and their means were calculated for further analysis.
Reliability tests were performed on the right sides of masseter muscles. Tests were performed by 2 experienced operators (A and B). Following each evaluation, the site marked on each subject was cleaned, and the raters were blinded to the results during the tests. To determine intra-operator reliability test, operator A evaluated masseter muscle stiffness on 2 occasions 5 days apart. To determine inter-operator reliability, operators A and B evaluated muscle stiffness on the same day, with a 30 min rest period between evaluations. Figure 1 shows MyotonPRO measurements of masseter muscle stiffness.
STATISTICAL ANALYSIS:
All statistical analyses were performed using SPSS version 21.0 statistical software (SPSS Inc, Chicago, IL), with at P<0.05 defined as statistically significant. Intra- and inter-rater reliability were determined by calculating intraclass correlation coefficients (ICC) with 95% confidence intervals (CI), using a 2-way mixed effects model and a 2-way random effects model. Standard error of measurement (SEM) was calculated as standard deviation×(I-ICC)1/2 and minimal detectable change (MDC) as 1.96×SEM×(2)1/2. Systematic error [17] and the degree of agreement about reliabilities were determined using Bland-Altman plots. Differences in masseter muscle stiffness on the 2 sides, as well as differences in stiffness during relaxation and maximum bite force, were compared with paired t-tests.
Results
DEMOGRAPHIC INFORMATION:
The demographic characteristics of the 20 study subjects, including their mean±SD age, weight, height, and BMI, are presented in Table 1.
INTRA- AND INTER-RATER RELIABILITIES:
Reliability tests were performed by measuring masseter muscle stiffness on the dominant side while in a relaxed condition using the MyotonPRO (Table 2). Mean stiffness assessed by operators A and B on the same day was 369.5 N/m and 387.4 N/m, respectively, whereas mean stiffness determined by operator A 5 days later was 350.2 N/m. Intra-operator reliability was good, with an ICC of 0.78, whereas inter-operator reliability was excellent, with an ICC of 0.95. All minimal detectable changes were >58.8. Bland-Altman plots showed that, for the intra-reliability test, the mean difference was 17.95 N/m and the 95% limits of agreement (LOAs) were −147.9 to 183.8 N/m (Figure 2A); whereas, for the inter-reliability test, the mean difference was −19.2 N/m, and the 95% LOAs were −92.9 to 54.5 N/m (Figure 2B).
DIFFERENCES IN MASSETER MUSCLE STIFFNESS UNDER DIFFERENT CONDITIONS:
The MyotonPRO can also be used to quantify differences in masseter muscle stiffness under different conditions (Figure 3). The mean stiffness of the masseter muscle on the dominant side was 369.5 N/m under relaxed conditions and 618.3 N/min at maximum bite force, an increase of 67.4% (Table 3).
DIFFERENCES IN MASSETER MUSCLE STIFFNESS ON THE RIGHT AND LEFT SIDES:
Mean masseter muscle stiffness under relaxed conditions was 369.5 N/m on the right side and 347.5 N/m on the left side, a difference that was not statistically significant (P>0.05) (Table 3). At maximum bite force, mean masseter muscle stiffness was 618.3 N/min on the right side and 607.1 N/m on the left side (P>0.05).
Discussion
INTRA- AND INTER-RATER RELIABILITIES:
To our knowledge, this study is the first to assess the reliability of MyotonPRO measurements of masseter muscle stiffness. We found that the intra-operator reliability was good and the inter-operator reliability was excellent, indicating that the MyotonPRO was reliable in assessing masseter muscle stiffness in a healthy population. The MyotonPRO has also been shown reliable in evaluating skeletal muscle stiffness. For example, the Myotonometer showed good intra-observer reliability (ICC >0.72) in measurements of biceps and triceps brachii muscle stiffness in subjects with subacute stroke, but inter-observer reliability was not evaluated [18]. Moreover, the MyotonPRO showed high intra-observer reliability in measurements of quadriceps muscle tone in older subjects, with ICCs ranging from 0.7 to 0.9 [19]. The MyotonPRO also showed excellent intra- and inter-observer reliabilities in determinations of the test-retest reliability of upper trapezius stiffness, with both ICCs being 0.97 [13].
Other methods have been used to quantify masseter muscle stiffness in patients with masticatory myofascial pain. For example, SWE showed good reliability, with an ICC >0.75 [20]. The difference in reliability between previous studies and ours was likely due to differences in assessment techniques. We also found that the MDC, an indirect measure of reliability, was >58.8 N/m, with a smaller MDC indicating higher reliability. Our findings indicate that MyotonPRO has certain advantages in quantifying masseter muscle stiffness.
We found that inter-rater reliability was better than intra-rater reliability. The difference may have been due to the 5-day interval between intra-operator assessments. Reliability may have been affected by many factors during those 5 days, including differences in exercise and minor changes in the experimental environment. Additionally, the Bland-Altman plots, which can indicate the degree of consistency, showed good reliability [17]. The mean difference in intra-observer measurements was 17.95 N/m (95% LOA −147.9 to 183.8 N/m), comparable to the mean difference in inter-observer measurements (−19.2 N/m; 95% LOA −92.9 to 54.5 N/min).
MASSETER MUSCLE STIFFNESS UNDER DIFFERENT CONDITIONS:
Mean masseter muscle stiffness, as evaluated by MyotonPRO, was 369.5±94.9 N/m under relaxed conditions, but was 618.3±150.7, or 64.7% higher, at maximal contraction, with an MDC >58.8 N/m. Bite force is associated with the biomechanical characteristics of the masticatory muscles, including the masseter muscle [5,21]. The masseter muscles play an important part in balancing masticatory function [22]. The 64.7% increase in masseter muscle stiffness may enhance the stability of masticatory function during the modulation of bite forces. Moreover, changes in status were shown to alter other biomechanical properties of the masseter muscles. For example, ultrasound examination of children with unilateral posterior cross-bite showed that masseter muscle thickness correlated positively with bite force, with maximal bite force increasing thickness 23.1% [23]. EMG showed that fatigue was greater in subjects with TMD than in healthy controls, with the duration of masticatory muscle contraction affecting the activity of these muscles [24]. SWE also showed that masseter muscle stiffness was significantly greater in subjects with TMD than in control subjects [20]. Myoton-3 quantitation of contracted and relaxed facial muscles yielded findings similar to ours, with muscles being stiffer during contraction [25].
Taken together, these results indicate that the biomechanical properties of masseter muscles are influenced by the state of contraction. These findings may enable better understanding of the relationships between masticatory muscles and masticatory function. MyotonPRO evaluation of masseter muscle stiffness in relaxed conditions and at maximum bite force may be a reliable reference for future studies.
DIFFERENCE IN MASSETER MUSCLE STIFFNESS BETWEEN THE RIGHT AND LEFT SIDES:
Interestingly, masseter muscle stiffness did not differ significantly on the right and left sides, both under conditions of relaxation and at maximum bite force. Physiologically, the 2 sides of the masseter muscle should be equally involved in maintaining masticatory function. Similar findings were observed using other techniques. For example, SWE evaluation of healthy subjects showed no difference in masseter muscle stiffness on the 2 sides [26]. Additionally, masseter muscle thickness on both sides was found to be similar [27]. Unilateral chewing has been shown result in differences in the thickness and activities of the masseter muscles on the 2 sides [28], and unilateral mastication was associated closely with TMD [29]. Our findings suggested that chewing in healthy populations is not unilateral, preventing the development of TMD.
LIMITATIONS:
This study had several limitations. First, only healthy subjects were recruited, suggesting the need to evaluate masseter muscles in patients with pathological conditions. In addition, many factors may have affected assessments of masseter muscle stiffness; including the pressure needed to hold the MyotonPRO to the masseter muscle and muscle activity, which may have been affected by the timing or duration of exercise. Furthermore, the MyotonPRO evaluated stiffness at 1 point of each masseter muscle, but this point may not have been representative of overall muscle stiffness. Finally, the maximal contraction status of the masseter muscle was defined subjectively. Additional studies are therefore necessary to quantify the maximal contraction of the masseter muscles.
Conclusions
In conclusion, MyotonPRO is a novel technique with high reliability in quantifying masseter muscle stiffness under both relaxed conditions and at maximum bite force. The finding that stiffness was similar on both sides provides a reference for future studies.
Figures
 Figure 1. Measurements of masseter muscle stiffness.
Figure 1. Measurements of masseter muscle stiffness. 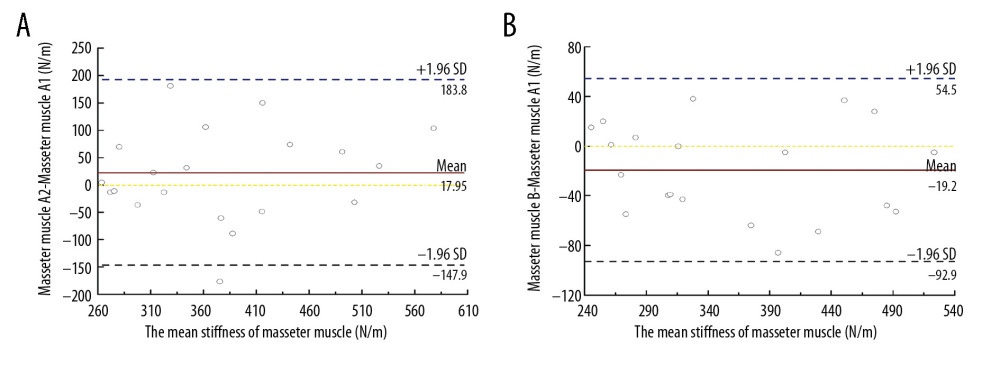 Figure 2. Bland-Altman plots of (A) intra-operator and (B) inter-operating reliabilities for assessing masseter muscle stiffness.
Figure 2. Bland-Altman plots of (A) intra-operator and (B) inter-operating reliabilities for assessing masseter muscle stiffness. 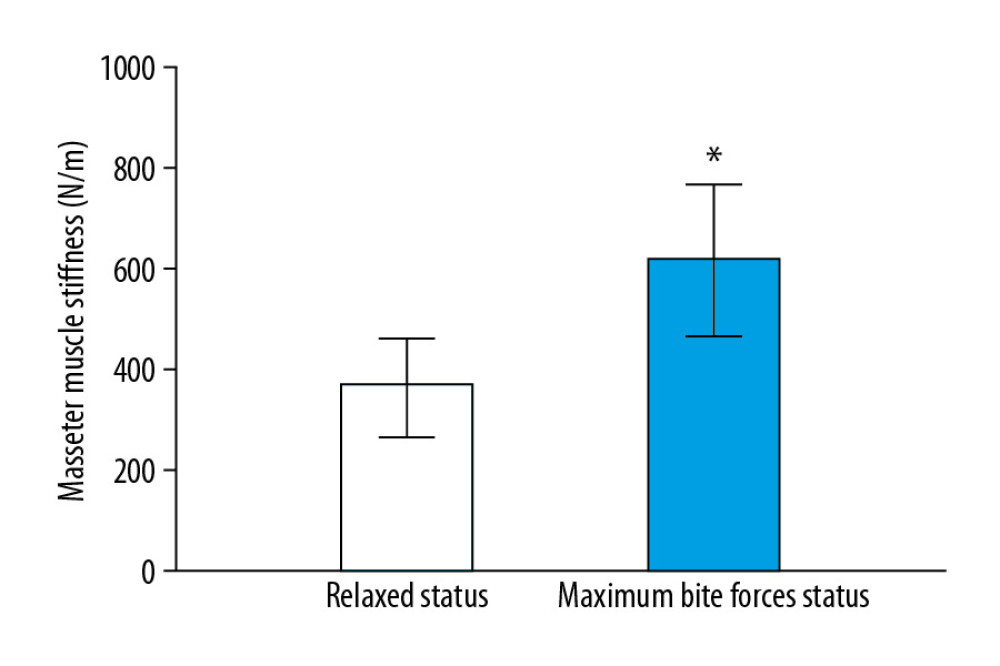 Figure 3. Mean±standard deviation masseter muscle stiffness under conditions of relaxation (white bar) and maximum bite force (blue bar). * P<0.05.
Figure 3. Mean±standard deviation masseter muscle stiffness under conditions of relaxation (white bar) and maximum bite force (blue bar). * P<0.05. References
1. Jenkins D, Temporomandibular disorders: J Am Dent Assoc, 2006; 137(10); 1360-61
2. Graber TM, Rakosi T, Petrovic AG, Functional analysis – examination of temporomandibular joint and condylar movement: Dentofacial orthopedics with functional appliances, 2009; 135-40, St. Louis, MO, Mosby
3. Armijo-Olivo S, Pitance L, Singh V, Effectiveness of manual therapy and therapeutic exercise for temporomandibular disorders: Systematic review and meta-analysis: Phys Ther, 2016; 96(1); 9-25
4. Canales GT, Guarda-Nardini L, Rizzatti-Barbosa CM, Distribution of depression, somatization and pain-related impairment in patients with chronic temporomandibular disorders: J Appl Oral Sci, 2019; 27; e20180210
5. Ingervall B, Helkimo E, Masticatory muscle force and facial morphology in man: Arch Oral Biol, 1978; 23(3); 203-6
6. Yoshimi T, Koga Y, Nakamura A, Mechanism of motor coordination of masseter and temporalis muscles for increased masticatory efficiency in mice: J Oral Rehabil, 2017; 44(5); 363-74
7. Weber P, Rodrigues Corrêa EC, de Paula Bolzan G, Chewing and swallowing in young women with temporomandibular disorder: Codas, 2013; 25(4); 375-80
8. Durham J, Newton-John TRO, Zakrzewska JM, Temporomandibular disorders: BMJ, 2015; 350; h1154
9. Suzuki S, Arima T, Kitagawa Y, Influence of glutamate-evoked pain and sustained elevated muscle activity on blood oxygenation in the human masseter muscle: Eur J Oral Sci, 2017; 125(6); 453-62
10. Woźniak K, Lipski M, Lichota D, Szyszka-Sommerfeld L, Muscle fatigue in the temporal and masseter muscles in patients with temporomandibular dysfunction: Biomed Res Int, 2015; 2015 269734
11. Disselhorst-Klug C, Schmitz-Rode T, Rau G, Surface electromyography and muscle force: Limits in sEMG-force relationship and new approaches for applications: Clin Biomech (Bristol, Avon), 2009; 24(3); 225-35
12. Huang J, Qin K, Tang C, Assessment of passive stiffness of medial and lateral heads of gastrocnemius muscle, Achilles tendon, and plantar fascia at different ankle and knee positions using the MyotonPRO: Med Sci Monit, 2018; 24; 7570-76
13. Liu CL, Feng YN, Zhang HQ, Assessing the viscoelastic properties of upper trapezius muscle: Intra- and inter-tester reliability and the effect of shoulder elevation: J Electromyogr Kinesiol, 2018; 43; 226-29
14. Feng YN, Li YP, Liu CL, Zhang ZJ, Assessing the elastic properties of skeletal muscle and tendon using shearwave ultrasound elastography and MyotonPRO: Sci Rep, 2018; 8(1); 17064
15. Walter SD, Eliasziw M, Donner A, Sample size and optimal designs for reliability studies: Stat Med, 1998; 17(1); 101-10
16. Gavronski G, Veraksits A, Vasar E, Maaroos J, Evaluation of viscoelastic parameters of the skeletal muscles in junior triathletes: Physiol Meas, 2007; 28(6); 625-37
17. Bland JM, Altman DG, A note on the use of the intraclass correlation coefficient in the evaluation of agreement between two methods of measurement: Comput Biol Med, 1990; 20(5); 337-40
18. Chuang LL, Wu CY, Lin KC, Lur SY, Quantitative mechanical properties of the relaxed biceps and triceps brachii muscles in patients with subacute stroke: A reliability study of the myoton-3 myometer: Stroke Res Treat, 2012; 2012 617694
19. Aird L, Samuel D, Stokes M, Quadriceps muscle tone, elasticity and stiffness in older males: Reliability and symmetry using the MyotonPRO: Arch Gerontol Geriatr, 2012; 55(2); e31-39
20. Takashima M, Arai Y, Kawamura A, Quantitative evaluation of masseter muscle stiffness in patients with temporomandibular disorders using shear wave elastography: J Prosthodont Res, 2017; 61(4); 432-38
21. Braun S, Bantleon HP, Hnat WP, A study of bite force, part 1: Relationship to various physical characteristics: Angle Orthod, 1995; 65(5); 367-72
22. Kuijpers MAR, Grefte S, Bronkhorst EM, Reduced masticatory function is related to lower satellite cell numbers in masseter muscle: Eur J Orthod, 2014; 36(3); 262-67
23. Castelo PM, Gavião MB, Pereira LJ, Bonjardim LR, Masticatory muscle thickness, bite force, and occlusal contacts in young children with unilateral posterior crossbite: Eur J Orthod, 2007; 29(2); 149-56
24. Ries LGK, Graciosa MD, Soares LP, Effect of time of contraction and rest on the masseter and anterior temporal muscles activity in subjects with temporomandibular disorder: Codas, 2016; 28(2); 155-62
25. Dietsch AM, Solomon NP, Sharkey LA, Perceptual and instrumental assessments of orofacial muscle tone in dysarthric and normal speakers: J Rehabil Res Dev, 2014; 51(7); 1127-42
26. Ewertsen C, Carlsen J, Perveez MA, Schytz H, Reference values for shear wave elastography of neck and shoulder muscles in healthy individuals: Ultrasound Int Open, 2018; 4(1); E23-29
27. Georgiakaki I, Tortopidis D, Garefis P, Kiliaridis S, Ultrasonographic thickness and electromyographic activity of masseter muscle of human females: J Oral Rehabil, 2007; 34(2); 121-28
28. Christensen LV, Mohamed SE, Bilateral masseteric contractile activity in unilateral gum chewing: Differential calculus: J Oral Rehabil, 1996; 23(9); 638-47
29. Yeler DY, Yılmaz N, Koraltan M, Aydin E, A survey on the potential relationships between TMD, possible sleep bruxism, unilateral chewing, and occlusal factors in Turkish university students: Cranio, 2017; 35(5); 308-14
Figures
Figure 1. Measurements of masseter muscle stiffness.Figure 2. Bland-Altman plots of (A) intra-operator and (B) inter-operating reliabilities for assessing masseter muscle stiffness.Figure 3. Mean±standard deviation masseter muscle stiffness under conditions of relaxation (white bar) and maximum bite force (blue bar). * P<0.05. Tables
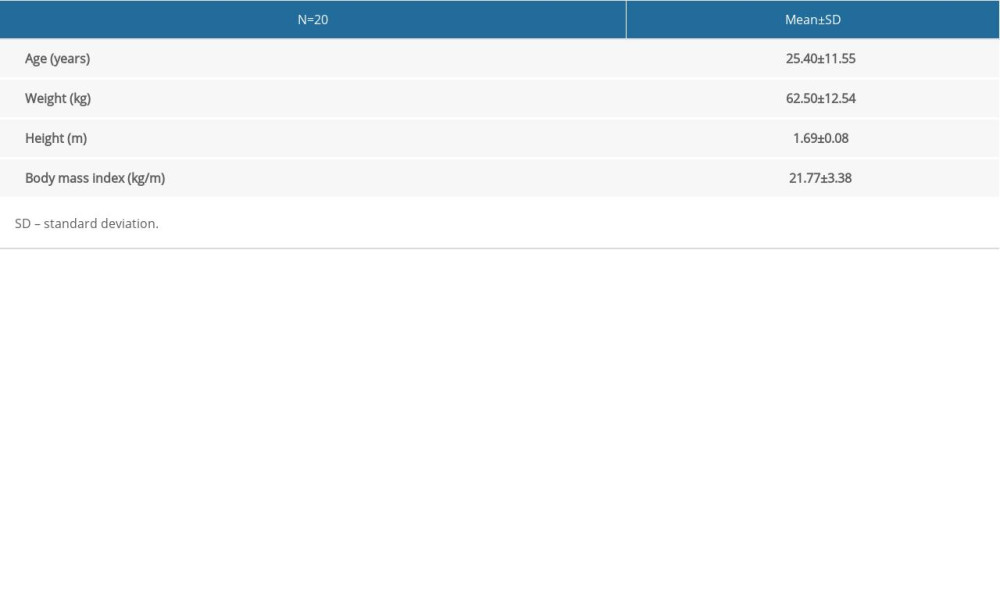 Table 1. Demographic characteristics of the study subjects. SD, standard deviation.
Table 1. Demographic characteristics of the study subjects. SD, standard deviation.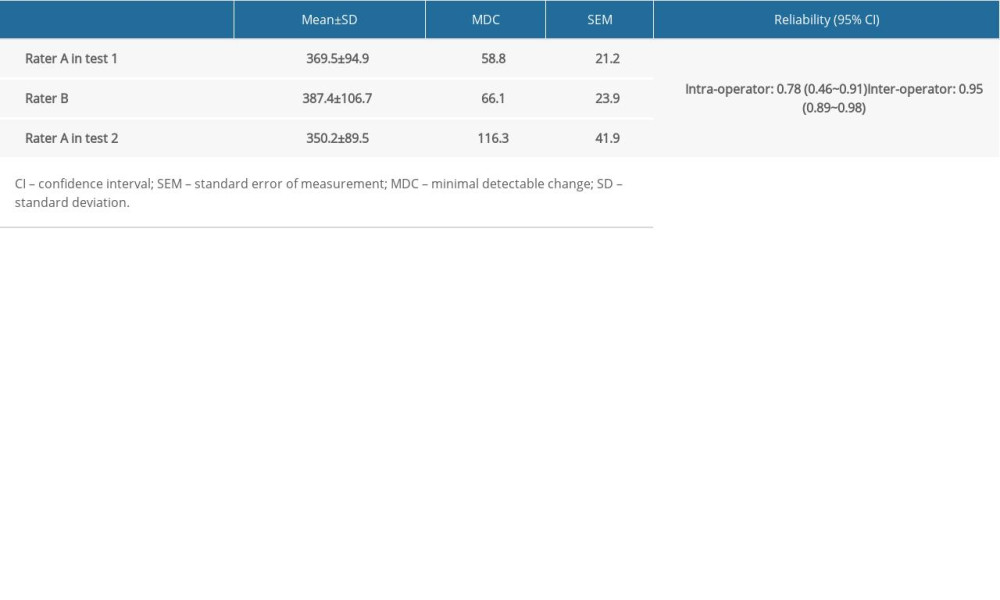 Table 2. Intra- and inter-rater reliabilities for assessing masseter muscle stiffness by MyotonPRO.
Table 2. Intra- and inter-rater reliabilities for assessing masseter muscle stiffness by MyotonPRO.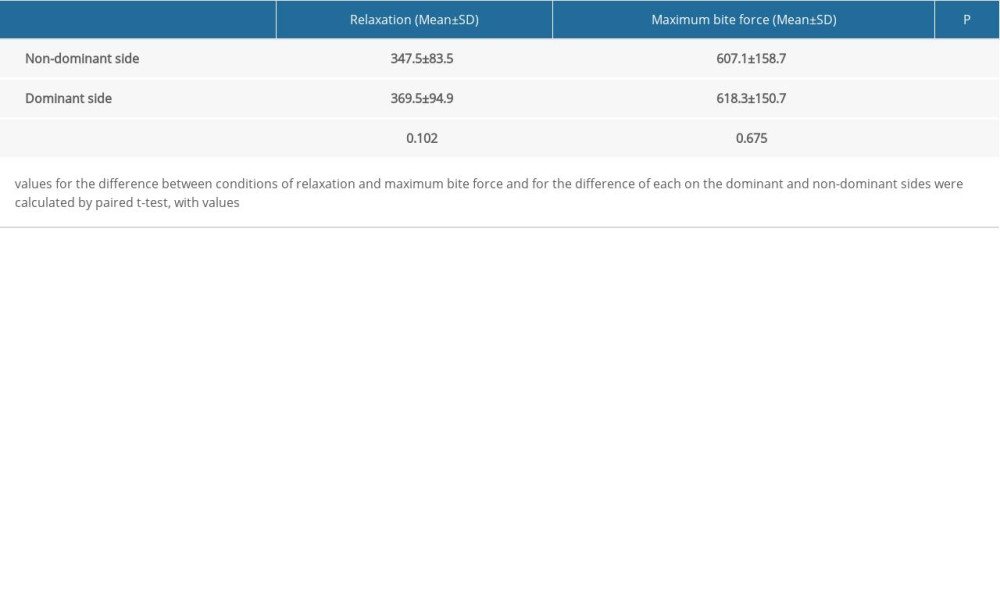 Table 3. Masseter muscle stiffness on both sides during conditions of relaxation and maximum bite force.Table 1. Demographic characteristics of the study subjects. SD, standard deviation.Table 2. Intra- and inter-rater reliabilities for assessing masseter muscle stiffness by MyotonPRO.Table 3. Masseter muscle stiffness on both sides during conditions of relaxation and maximum bite force.
Table 3. Masseter muscle stiffness on both sides during conditions of relaxation and maximum bite force.Table 1. Demographic characteristics of the study subjects. SD, standard deviation.Table 2. Intra- and inter-rater reliabilities for assessing masseter muscle stiffness by MyotonPRO.Table 3. Masseter muscle stiffness on both sides during conditions of relaxation and maximum bite force. In Press
Clinical Research
Effect of Dexmedetomidine Hydrochloride Nasal Spray on Anxiety and Sleep in Patients Undergoing Gynecologic...Med Sci Monit In Press; DOI: 10.12659/MSM.952465
Clinical Research
Prognostic Value of Mortality Scoring Systems in Patients With Severe Burns: Identifying Key Predictors of ...Med Sci Monit In Press; DOI: 10.12659/MSM.951713
Laboratory Research
Evaluation of the Trueness and Precision of Cast, Milled-Cast, Milled, and 3D-Printed Post-and-Core Techniq...Med Sci Monit In Press; DOI: 10.12659/MSM.953491
Clinical Research
Outcomes After Minimally Invasive Intramedullary Nail Fixation and Locking Plate Fixation Among Patients Wi...Med Sci Monit In Press; DOI: 10.12659/MSM.952670
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,214
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,757,839
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,153
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,809
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387