19 October 2020: Clinical Research
Objective Assessment of Regional Stiffness in Achilles Tendon in Different Ankle Joint Positions Using the MyotonPRO
Tian-Tian Chang1BEF, Ya-Nan Feng2BDF, Yi Zhu3CDF, Chun-Long Liu4ABC, Xue-Qiang Wang1ACD, Zhi-Jie Zhang2ADE*DOI: 10.12659/MSM.926407
Med Sci Monit 2020; 26:e926407






Abstract
BACKGROUND: Achilles tendinopathy commonly occurs in specific regions of the tendon, and Achilles tendon stiffness can be related to local pathological changes in the tendon. The MyotonPRO is a new handheld device that conveniently assesses stiffness of muscles and tendons. This study aimed to 1) evaluate the intra- and inter-rater reliability of stiffness measurements of the Achilles tendon at different ankle positions, 2) investigate the modulation of stiffness at different ankle joint angles, and 3) examine the differences between 2 regions of Achilles tendon stiffness.
MATERIAL AND METHODS: Thirty healthy young adults (15 men and 15 women) participated in this study. The regional Achilles tendon stiffness at 0 cm (AT-0) and 6 cm (AT-6) above the tendon insertion were evaluated by the MyotonPRO in the neutral position and 10° dorsiflexion of the ankle joint. Measurements of stiffness were taken by 2 raters on the first day and 5 days later. The stiffness data were compared by repeated measures analysis of variance (ANOVA).
RESULTS: The intra- and inter-rater reliability of stiffness measurements at AT-0 and AT-6 for each ankle position were good (all intraclass correlation coefficients >0.84). A significant modulation of Achilles tendon stiffness was obtained at different ankle joint angles (P<0.05). Stiffness at AT-0 was higher than at AT-6 (P<0.05) in both positions.
CONCLUSIONS: These results suggest the MyotonPRO reliably assessed Achilles tendon stiffness and monitors its modulation, and tendon stiffness increased with ankle dorsiflexion. Stiffness was also nonuniform along the length of the tendon.
Keywords: Achilles Tendon, Elastic Tissue, Mechanical Phenomena, Ankle Joint, Muscle, Skeletal, Range of Motion, Articular, Tendinopathy
Background
The Achilles tendon is a compliant tendon with an important function of storing and releasing elastic strain energy during locomotion [1]. Stiffness is one of the mechanical property parameters of muscles and tendons affecting muscle power and the rate of muscle force production [2]. Muscle and tendon stiffness is related to the condition of the tissue, such as pain [3], fatigue [4], and cramps [5]. Therefore, it is important to investigate the modulation of Achilles tendon stiffness under different conditions.
Ankle and foot overuse injuries frequently cause Achilles tendinopathy, which has an incidence rate of 0.2% in the general population [6]. The 2 main types of Achilles tendinopathy are insertional tendinopathy at the calcaneus-Achilles tendon junction and noninsertional tendinopathy, which occurs 2 cm to 6 cm proximal to the insertion of the tendon into the calcaneus [7]. These local lesions can cause the modulation of tendon mechanical properties [8]. It is also possible that changes in localized tendon compliance can alter the deformation patterns of adjacent tissue, thereby risking localized tissue injury. Measuring Achilles tendon stiffness is useful for assessing the pathology of the tendon [9]. A significantly lower shear modulus of the Achilles tendon is associated with tendinopathy [10] and tendon fracture [11]. Several studies on Achilles tendon stiffness have been reported, and the stiffness measurement of the whole tendon was quantified in previous studies [12]. In terms of anatomy, the Achilles tendon is nonuniform, and the cross-sectional area of the tendon varies along its length. The elongation of different regions of the tendon is modulated under the same force [13]. More importantly, pathology commonly occurs in a specific region of the tendon. Therefore, it is necessary to quantify the regional stiffness of the Achilles tendon.
Recently, the MyotonPRO has been used to assess the mechanical properties of soft tissues, including muscles and tendons [14–16]. The MyotonPRO is a new noninvasive, easy-to-operate, handheld device used to conveniently and quickly assess the stiffness of muscles and tendons. Soft tissue stiffness has been evaluated as shear modulus by shear wave elastography in past years. Although shear wave elastography is an excellent tool which provides a technique to quickly assess the stiffness of muscle and tendon, its required technical expertise and high cost limit its wide clinical application. Our previous studies have demonstrated that the MyotonPRO is a reliable method to quantify the stiffness of the medial head of the gastrocnemius, lateral head of the gastrocnemius [14], Achilles tendon [15], and upper trapezius [16] in healthy populations. In addition, we found a significant correlation between the stiffness of the gastrocnemius muscle and Achilles tendon measured by the MyotonPRO and the shear modulus as quantified by shear wave elastography [14]. Therefore, we believe the MyotonPRO can also be used to evaluate Achilles tendon stiffness at different ankle joint angles.
The aims of the present study were to 1) quantify the intra-and inter-rater reliability of the Achilles tendon stiffness measurements using the MyotonPRO; 2) assess the differences in Achilles tendon stiffness at different angles of the ankle joint; and 3) evaluate the variation of stiffness at different regions of the Achilles tendon.
Material and Methods
ETHICS:
This study received approval by the Human Subjects Ethics Committee of Luoyang Orthopedic Hospital of Henan Province (No. 2019-001-01). All participants were informed of the procedures of this experiment and gave their written informed consent before participating in the trial. All of the experimental procedures adhered to the principles of the Declaration of Helsinki.
PARTICIPANTS:
This was a single-center study with 30 participants (15 men and 15 women; age 23.4±4.2 years; body mass index (BMI) 20.6±2.7 kg/m2) recruited from the Rehabilitation Therapy Center of the Henan Province Orthopedic Hospital. Healthy participants were included if they met the following criteria: 1) age was >18 years and <30 years; 2) BMI was ≥16 kg/m2 or ≤28 kg/m2; 3) they did not have musculoskeletal system diseases; 4) they did not have any Achilles tendon dysfunction; 5) they did not have skin lesions above the measuring regions; 6) they did not perform regular exercise; and 7) they could complete the entire experiment.
EQUIPMENT:
The MyotonPRO (MyotonAS, Tallinn, Estonia) was used to evaluate Achilles tendon stiffness. The probe of the MyotonPRO generated mechanical impulses via an electromagnetic mechanism after precompression of the subcutaneous tissues [17]. The impulses cause oscillations of the skin and underlying muscle or fascia. Consecutive oscillations were recorded by the device’s accelerometer. Five parameters that provide quantitative information about the mechanical properties of tissues were computed by the MyotonPRO. One of these parameters is stiffness [N/m], which represents the capability of tissue to resist external, deforming forces. The stiffness value was calculated as the maximum acceleration of oscillation/maximum displacement of the tissue. A higher stiffness value indicated greater stiffness of tissue. The multi-scan mode, consisting of 5 single impulses with 0.8 s intervals, was used [18].
PROCEDURES:
All measurements were carried out in the same room with a temperature of approximately 25°C. Participants were placed in a prone position with the hip and knee joint fully extended on the examination couch, and they were instructed to completely relax. All the measures were performed on the dominant limb. The dominant leg of the subject was determined by which side of the lower limbs was used to kick a ball [19,20]. The stiffness of the Achilles tendon was measured at the neutral position (ankle joint dorsiflexion 0°) and at 10° dorsiflexion of the ankle joint. The measurement regions for the stiffness of the tendon were located at 0 cm (AT-0) and 6 cm (AT-6) above the tendon insertion (calcaneal tuberosity) [21]. The 2 points of the tendon were marked by the same physical therapist. Passive ankle joint at 10° dorsiflexion and the neutral position were maintained by a self-made splint (Figure 1). The angle of the ankle joint was measured with a goniometer. Konor et al. (2012) demonstrated good reliability (intraclass correlation coefficient (ICC) >0.85) of a goniometer in measuring the ankle dorsiflexion range of motion [22]. The probe of the MyotonPRO was placed on and perpendicular to the Achilles tendon surface, overlying the tendon of interest. Stiffness at AT-0 and AT-6 was measured with 0° and 10° dorsiflexion by the MyotonPRO.
Measurements of stiffness were taken on 2 occasions: on the first day and 5 days later. One rater (CTT) evaluated the stiffness of AT-0 and AT-6 with the ankle in the neutral position and then 10° dorsiflexion. Then, the participants relaxed for 30 min. The entire session was repeated by the second rater (ZJ), following the same steps. The order of the raters was always rater 1 (CTT) performing the first measurement and rater 2 (ZJ) performing the second. The raters were blinded to the results during the test. Participants were instructed to continue with their normal routine, and then 5 days later, rater 1 (CTT) repeated the measurements. The 2 raters were trained to use the MyotonPRO in a formal training course.
STATISTICAL ANALYSIS:
Statistical analysis was performed using SPSS software (SPSS version 22.0, IBM, Armonk, NY, USA). Stiffness data are presented as mean±standard deviation (SD). The Shapiro-Wilk test was used to assess the normal distribution of the data. The participant demographics were calculated using descriptive statistics. Bland-Altman plots that visually present intra-rater and inter-rater reliability were made by MedCalc 18 software (Software Biba, Ostend, Belgium). Histograms representing group differences were created by GraphPad Prism 8. The ICC was computed using ICC (2,2) and ICC (3,1) models, and were used to evaluate the reliability of the test. The value of ICC was interpreted by the Domholdt scale [23]: <0.25=poor; 0.26–0.49=low; 0.50–0.69=moderate; 0.70–0.89=high; and 0.90–1.00=very high. The standard error of measurement (SEM) and the minimal detectable change (MDC) were calculated by the following formula: SEM=standard deviation ×√1-ICC; MDC=1.96×SEM×√2. A 2-way mixed model repeated measures analysis of variance (ANOVA) (2 ankle positions×2 tendon regions) and Bonferroni’s post hoc test were utilized to study the effect of ankle angle and tendon region on Achilles tendon stiffness. The significance level was P<0.05 for all tests.
Results
INTRA- AND INTER-RATER RELIABILITY:
The reliability results of the Achilles tendon measurements taken at the ankle joint 0° and dorsiflexion 10° in the dominant limb are presented in Tables 1 and 2, respectively. The values of ICC were high to very high, ranging from 0.89 to 0.93 in the ankle neutral position (AT-0: ICCA1B=0.93, ICCA1A 2=0.92; AT-6: ICCA1B=0.89, ICCA1A2=0.93). The values of ICC were high to very high with a range from 0.85–0.92 in the ankle joint 10° dorsiflexion (AT-0: ICCA1B=0.94, ICCA1A2=0.92; AT-6: ICCA1B=0.85, ICCA1A2=0.87). According to the value of ICC by the Domholdt scale [23], all reliability values for the measurements of Achilles tendon stiffness were high (ICC >0.84).
Bland-Altman plots for intra- and inter-rater reliability of AT-0 and AT-6 stiffness in different ankle positions are presented in Figure 2. For intra-rater reliability of AT-0 stiffness in the ankle neutral position and 10° dorsiflexion, the mean difference was 3.00 and 17.7 N/m, respectively, and the inter-rater reliability was 8.20 and 10.70 N/m, respectively. For intra-rater reliability of AT-6 stiffness in the ankle neutral position and 10° dorsiflexion, the mean difference was −7.90 and 12.30 N/m, respectively, and the inter-rater reliability was −8.30 and 22.20 N/m, respectively.
DIFFERENCES IN ACHILLES TENDON STIFFNESS AT 2 POSITIONS/REGIONS:
Figure 3 shows the Achilles tendon stiffness changes at AT-0 and AT-6 in 0° passive ankle rotation and 10° dorsiflexion. The differences in Achilles tendon stiffness were compared in a 2-way repeated measures ANOVA, and the results revealed a significant main effect of ankle position (F=56.86, P<0.01) and tendon region (F=43.23, P<0.01), but with no interaction (F=2.20, P=0.14). AT-0 and AT-6 stiffness was significantly higher with 10° dorsiflexion than in the neutral position. Additionally, the Achilles tendon stiffness at AT-0 was always greater than at AT-6, regardless of whether the ankle joint was in the neutral position or 10° dorsiflexion.
Discussion
INTRA- AND INTER-RATER RELIABILITY:
The results of the present study demonstrate the excellent intra- and inter-rater reliability of the MyotonPRO in measuring Achilles tendon stiffness at the ankle neutral position and 10° dorsiflexion. These results were similar to our previous study, in which we reported the reliability of MyotonPRO in measuring Achilles tendon stiffness [15]. Ko et al. (2018) showed that the SEM of stiffness in the mid-position of the Achilles tendon in patients with chronic spinal cord injury was less than 104 N/m and reported ICCs ranging from 0.81 to 0.84, but they did not examine the inter-rater reliability of the MyotonPRO [24]. In our previous study, the measured location of the Achilles tendon stiffness was 4 cm above the calcaneal tuberosity, and the ICCs of intra- and inter-rater reliability in the dominant leg were 0.9 and 0.95, respectively [15]. Our present findings suggest that the reliability of the stiffness measurements differed between the evaluated joint positions and tendon regions. Other studies have confirmed the variation in the reliability of the MyotonPRO in different muscle groups and positions [25,26]. Taş et al. (2019) quantified the stiffness of the Achilles tendon with the ankle joint at 0° and 10° dorsiflexion (measurement region was 2 cm above the calcaneal tuberosity), and they found excellent MyotonPRO inter-and intra-rater reliability (ICC: 0.87–0.94), with a corresponding SEM of less than 44 N/m and MDC less than 122 N/m [27]. In summary, there is consensus that the MyotonPRO is a credible device for assessing passive Achilles tendon stiffness.
Figure 2 shows the consistency of our results. Regardless of the different regions and positions tested, almost all of the measurements were distributed within the 95% confidence interval. Although the mean values differed from 0, the error within the limits of agreement was acceptable [28].
THE MODULATION IN ACHILLES TENDON STIFFNESS AT DIFFERENT ANGLES:
As seen in Figure 3, the stiffness of the Achilles tendon in 10° dorsiflexion was significantly higher than that in the neutral ankle joint position. This result is consistent with a previous study which found that the Achilles tendon became stiffer after stretching [27]. Shan et al. (2019) demonstrated that the stiffness of the medial head of the gastrocnemius and medial and lateral soleus was correlated with ankle joint position or muscle contraction [29]. Further, there was a significant increase in shear modulus of the medial head of the gastrocnemius and the lateral head of the gastrocnemius in the lengthened muscle position [26,30]. These cases demonstrate the straining-stiffness behavior of muscles and tendons after the fibers become tight [31]. Many studies identified the stiffness of muscle in a tension state, but only a few studies focused on the change of tendon stiffness after stretching [29,30]. When the tendons and muscles respond to the same mechanical load, such as tension, they may have different stiffness modulation [32]. Sébastien et al. (2013) measured the difference between Achilles tendon stiffness and stiffness of the medial gastrocnemius and confirmed that the extent of increase in tendon stiffness was greater than that of muscle [33].
In the present study, changing from the ankle neutral position to 10° dorsiflexion resulted in an increase of 17.35% and 16.87% in stiffness at AT-0 and AT-6, respectively. Our previous study reported an increase of 13.9% in Achilles tendon stiffness (measurement site: 4 cm above the calcaneal tuberosity) from the ankle neutral position (1143 N/m) to 30° dorsiflexion (1329 N/m) in a healthy population [15]. Using the MyotonPRO, Taş et al. (2019) revealed that the stiffness of the Achilles tendon (measurement region: 2 cm above the calcaneal tuberosity) was increased by 40% at the ankle 10° dorsiflexion position compared to the ankle neutral position, and they found the effect of joint position on tendon stiffness varied greatly according to participant’s personal characteristics [27]. Sébastien et al. (2013) examined the difference in Achilles tendon stiffness (measurement region: 5 cm above the calcaneal tuberosity) between the ankle neutral position and the ankle maximum dorsiflexion position by transient shear wave elastography and found Achilles tendon stiffness at ankle maximum dorsiflexion was 5 times that of the stiffness of the ankle in the neutral position, increasing from 147 kPa to 780 kPa, respectively [33]. Thus, potential reasons for different measurements may include the heterogeneity of the Achilles tendon, potential differences between different regions, different measurement methodologies, and differences in the participants being studied.
DIFFERENCES OF ACHILLES TENDON STIFFNESS IN THE 2 REGIONS:
We found significant heterogeneity in Achilles tendon stiffness along its length, suggesting that the stiffness near the insertion on the Achilles tendon, AT-0, is greater than that near the muscle-tendon junction, AT-6, regardless of the ankle joint position. Interestingly, the increased rate of stiffness was similar in the 2 measured regions. The stiffness of AT-0 was 30.96% higher than the stiffness of AT-6 in the ankle neutral position, and 31.24% higher than in the 10° dorsiflexion position.
Similar nonuniform mechanical behaviors have been found in other studies. Some researchers observed that there are differences in displacement across the tendon thickness. For example, Arndt et al. (2012) investigated the different displacement between the superficial, middle, and deep layers of the Achilles tendon during passive stretch and found the displacement of the superficial Achilles tendon was always less than that of the deeper portions of the tendon [34]. Similarly, Slane et al. (2014) confirmed the same spatial variations in tendon deformation among different layers of the Achilles tendon in eccentric plantar flexor loading and passive stretch [35]. In addition, studies have focused on nonuniform deformation along the Achilles tendon axis. Arampatzis et al. (2005) [36] and Finni et al. (2003) [37] showed the differences in elongation between the tendon and the aponeurosis under the same external load and discovered spatial variations of tendon deformation. This finding is similar to the result from a study using a 3D model of the Achilles tendon to observe that the displacement near the proximal aspect is greater than that at the calcaneal insertion of the tendon [38]. Age is associated with nonuniform displacement of the Achilles tendon. Slane et al. (2015) discovered that regional nonuniformity was lower in middle-aged participants than in young participants [39]. The Achilles tendon is composed of the gastrocnemius tendon and the soleus tendon in a spiral manner, which may contribute to nonuniform elongations [40,41]. Handsfield et al. (2016) reported that the main factors causing displacement nonuniformity between tendon regions were intra-tendon sliding and differential muscle forces [38]. The variations of regional deformation in the Achilles tendon may be related to the force transmission and elastic storage during muscle contraction [42].
In previous studies, the nonuniform displacement and stress variation of the Achilles tendon has been observed under the same stretch force [35,43]. Achilles tendon stiffness may differ along the axis. Some studies used the parameter of the shear wave speed to highlight nonuniform Achilles tendon stiffness. Slane et al. (2017) evaluated shear wave speed heterogeneity over the length of the Achilles tendon [44]. Dewall et al. (2014) assessed the shear wave speed at different muscle-tendon regions by supersonic shear imaging and found spatial differences of shear wave speed from the free tendon to the gastrocnemius aponeurosis, agreeing with the idea that the aponeurosis is more compliant than the free tendon in healthy young participants [31]. Consistent with our present results, Coombes et al. (2017) used the method of simple surface-wave elastography to assess the nonuniform stiffening of the Achilles tendon and found that the shear wave velocity gradually decreases along the axis of the Achilles tendon in different ankle dorsiflexion angles [43]. In our present study, the nonuniform stiffness of the Achilles tendon may have been because the AT-0 attached to the calcaneal tuberosity, a stiff and fixed structure, whereas the AT-6 attached near the gastrocnemius muscle, a soft and compliant structure. Reeves et al. (2017) suggested that the more compliant proximal portion may act as a mechanical buffer, protecting the stiffer tissue in the distal portion of the Achilles tendon from injury [41]. The complex pattern of mechanical properties within the Achilles tendon may be designed to minimize the risk of Achilles tendon injury and strengthen its function.
LIMITATIONS:
There are several limitations to this study. First, despite the marking method of the MyotonPRO measurement location by the same therapist, a waterproof marker was not used to ensure the same placement on the 2 days. Second, although our team suggested that participants should be relaxed during the whole experiment, this could not be precisely controlled without the use of electromyography. In addition, the goniometer was not tested for reliability in this study. Finally, we evaluated Achilles tendon stiffness of only healthy subjects. Therefore, future experiments should focus on assessing stiffness modulations of Achilles tendinopathy.
Conclusions
The MyotonPRO is reliable for evaluating stiffness at the different regions and positions of the Achilles tendon. The stiffness of the Achilles tendon was increased with ankle dorsiflexion. Nonuniform behavior was consistently present within the Achilles tendon at the ankle neutral position and dorsiflexion. Further research is needed to investigate stiffness in people with Achilles tendinopathy.
Figures
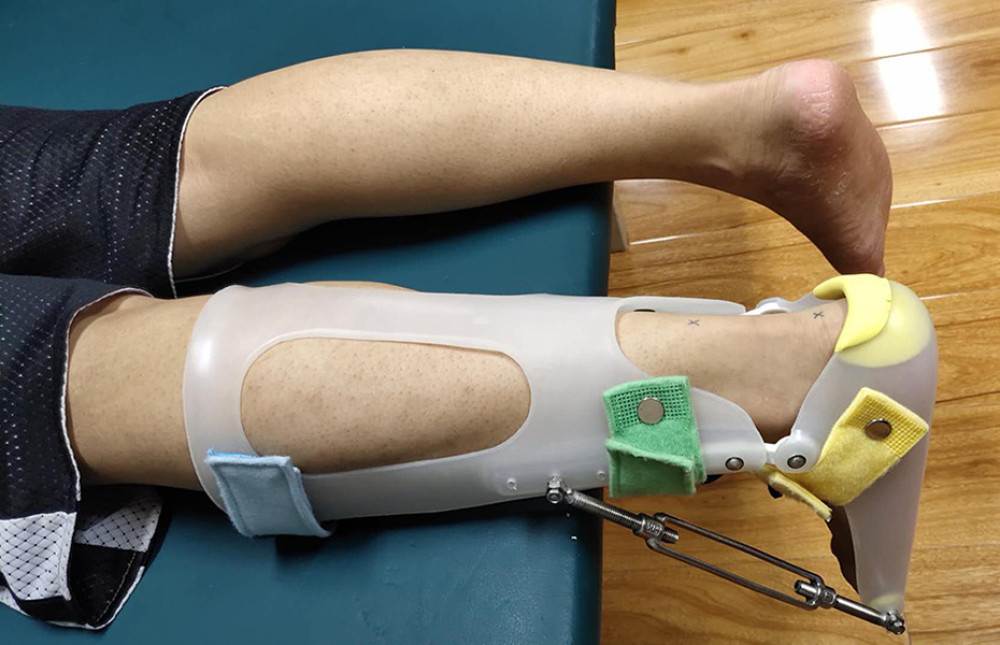 Figure 1. Photograph of the splint.
Figure 1. Photograph of the splint. 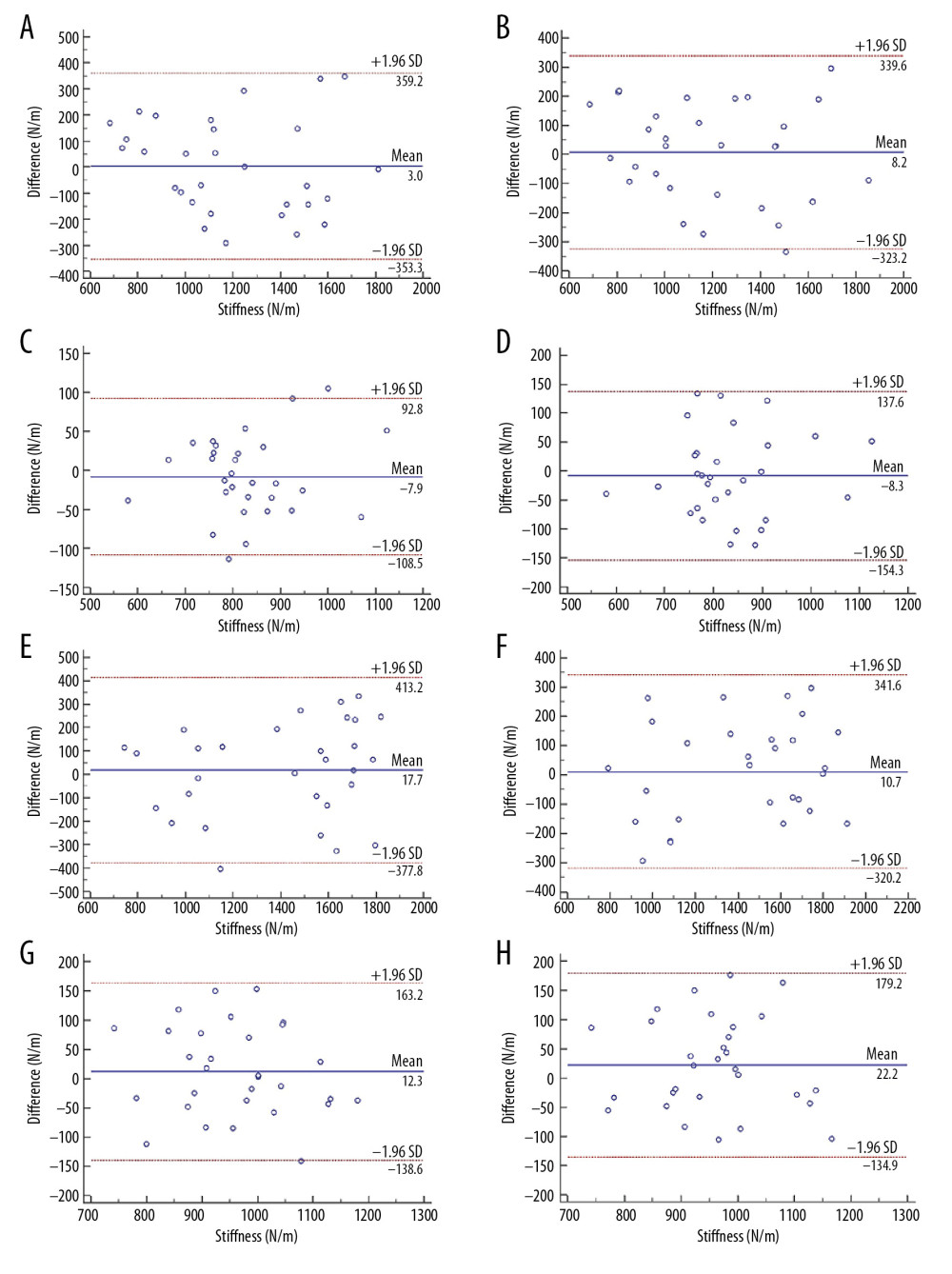 Figure 2. Bland-Altman plots of intra- and inter-rater reliability of Achilles tendon stiffness. (A, B) Intra- and inter-rater reliability of AT-0 stiffness at ankle neutral position. (C, D) Intra and inter-rater reliability of AT-6 stiffness at ankle neutral position. (E, F) Intra- and inter-rater reliability of AT-0 stiffness at ankle dorsiflexion 10°. (G, H) Intra- and inter-rater reliability of AT-6 stiffness at ankle dorsiflexion 10°.
Figure 2. Bland-Altman plots of intra- and inter-rater reliability of Achilles tendon stiffness. (A, B) Intra- and inter-rater reliability of AT-0 stiffness at ankle neutral position. (C, D) Intra and inter-rater reliability of AT-6 stiffness at ankle neutral position. (E, F) Intra- and inter-rater reliability of AT-0 stiffness at ankle dorsiflexion 10°. (G, H) Intra- and inter-rater reliability of AT-6 stiffness at ankle dorsiflexion 10°. 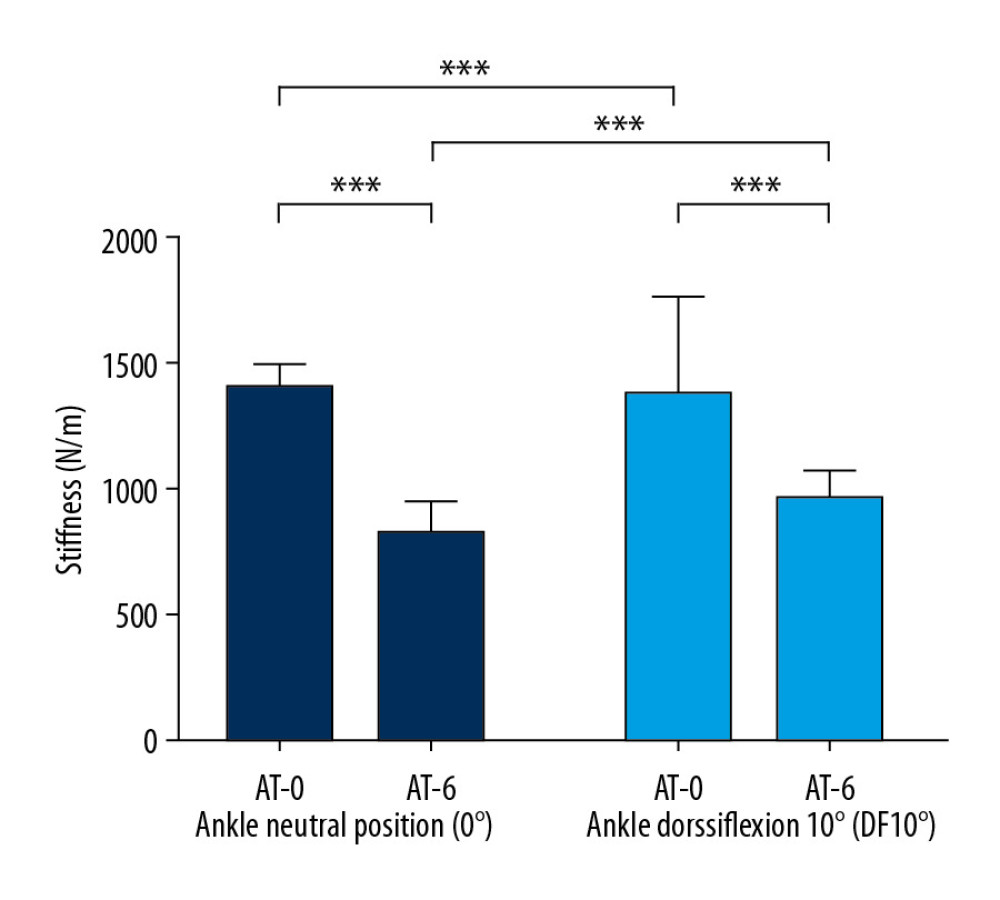 Figure 3. The mean stiffness of AT-0 and AT-6 at ankle joint 0° (deep blue) and dorsiflexion 10° (light blue). The difference between AT-0 and AT-6 mean stiffness at 0° and dorsiflexion 10°. *** P<0.001.
Figure 3. The mean stiffness of AT-0 and AT-6 at ankle joint 0° (deep blue) and dorsiflexion 10° (light blue). The difference between AT-0 and AT-6 mean stiffness at 0° and dorsiflexion 10°. *** P<0.001. Tables
Table 1. Inter-and intra-operator reliability of Achilles tendon at the neutral ankle neutral. ICC, intraclass correlation coefficients; CI, confidence interval; SEM (N/m), the standard error of measurement; MDC (N/m), the minimal detectable change; A1B, inter-rater reliability; A1A2, intra-rater reliability. Table 2. Inter-and intra-operator reliability of Achilles tendon at the ankle 10° dorsiflexion. ICC, intraclass correlation coefficients; CI, confidence interval; SEM(N/m), the standard error of measurement; MDC(N/m), the minimal detectable change; A1B, inter-rater reliability; A1A2, intra-rater reliability.
Table 2. Inter-and intra-operator reliability of Achilles tendon at the ankle 10° dorsiflexion. ICC, intraclass correlation coefficients; CI, confidence interval; SEM(N/m), the standard error of measurement; MDC(N/m), the minimal detectable change; A1B, inter-rater reliability; A1A2, intra-rater reliability.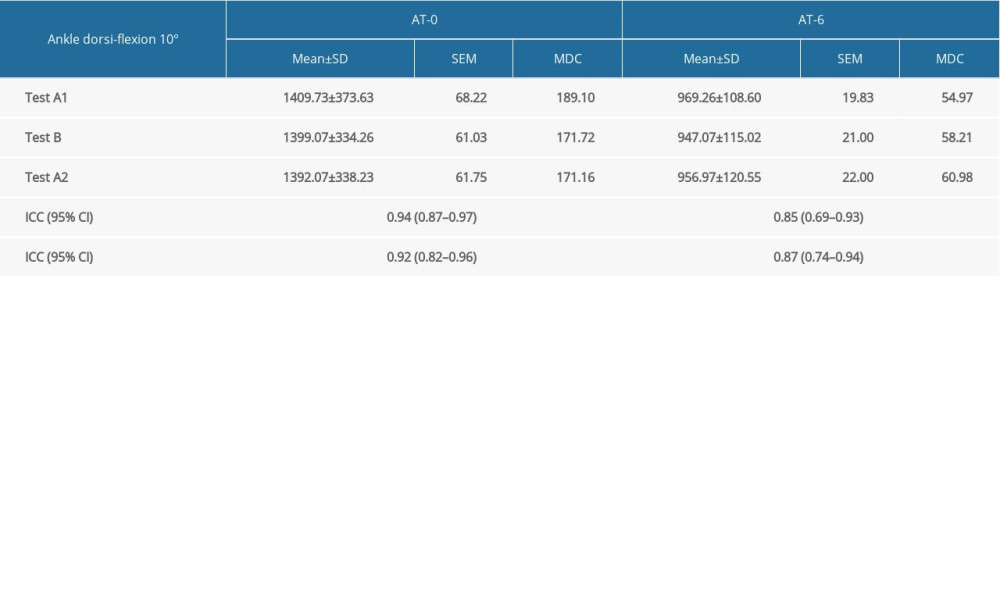
References
1. Obst SJ, Newsham-West R, Barrett RS, Changes in Achilles tendon mechanical properties following eccentric heel drop exercise are specific to the free tendon: Scand J Med Sci Sports, 2016; 26; 421-31
2. Morgan GE, Martin R, Williams L, Objective assessment of stiffness in Achilles tendinopathy: A novel approach using the Myotonpro: BMJ Open Sport Exer Med, 2018; 4; e000446
3. Zhang ZJ, Ng GY, Lee WC, Fu SN, Changes in morphological and elastic properties of patellar tendon in athletes with unilateral patellar tendinopathy and their relationships with pain and functional disability: PLoS One, 2014; 9; e108337
4. Andonian P, Viallon M, Le Goff , Shear-wave elastography assessments of quadriceps stiffness changes prior to, during and after prolonged exercise: A longitudinal study during an extreme mountain ultra-marathon: PLoS One, 2016; 11; e0161855
5. Lee SS, Gaebler-Spira D, Zhang LQ, Use of shear wave ultrasound elastography to quantify muscle properties in cerebral palsy: Clin Biomech (Bristol, Avon), 2016; 31; 20-28
6. Romero-Morales C, Martín-Llantino P, Calvo-Lobo C, Comparison of the sonographic features of the Achilles tendon complex in patients with and without Achilles tendinopathy: A case-control study: Phys Ther Sport, 2019; 35; 122-26
7. Almekinders LC, Temple JD, Etiology, diagnosis, and treatment of tendonitis: An analysis of the literature: Med Sci Sport Exer, 1998; 30; 1183-90
8. Obst SJ, Heales LJ, Schrader BL, Are the mechanical or material properties of the achilles and patellar tendons altered in tendinopathy? A systematic review with meta-analysis: Sports Med, 2018; 48(9); 2179-98
9. Zordo TD, Chhem R, Smekal V, Real-time sonoelastography: Findings in patients with symptomatic Achilles tendons and comparison to healthy volunteers: Ultraschall Med, 2009; 31; 394-400
10. Coombes BK, Tucker K, Vicenzino B, Achilles and patellar tendinopathy display opposite changes in elastic properties: A shear wave elastography study: Scand J Med Sci Sports, 2018; 28(3); 1201-8
11. Frankewycz B, Penz A, Weber J, Achilles tendon elastic properties remain decreased in long term after rupture: Knee Surg Sports Traumatol Arthrosc, 2018; 26; 2080-87
12. Seynnes OR, Bojsen-Møller J, Albracht K, Ultrasound-based testing of tendon mechanical properties: A critical evaluation: J Appl Physiol, 2015; 2(118); 133-41
13. Wren TA, Yerby SA, Gary S, Beaupré , Mechanical properties of the human Achilles tendon: Clin Biomech, 2001; 16(3); 245-51
14. Feng YN, Li YP, Liu CL, Assessing the elastic properties of skeletal muscle and tendon using shearwave ultrasound elastography and MyotonPRO: Sci Rep, 2018; 8; 17064
15. Liu CL, Li YP, Wang XQ, Quantifying the stiffness of achilles tendon: Intra- and inter-operator reliability and the effect of ankle joint motion: Med Sci Monit, 2018; 24; 4876-81
16. Liu CL, Feng YN, Zhang HQ, Assessing the viscoelastic properties of upper trapezius muscle: Intra- and inter-tester reliability and the effect of shoulder elevation: J Electromyogr Kinesiol, 2018; 43; 226-29
17. Drenth H, Zuidema SU, Krijnen WP, Psychometric properties of the Myotonpro in dementia patients with paratonia: Gerontology, 2018; 64; 401-12
18. Chen G, Wu J, Chen G, Reliability of a portable device for quantifying tone and stiffness of quadriceps femoris and patellar tendon at different knee flexion angles: PLoS One, 2019; 14; e0220521
19. Zhang ZJ, Ng GYF, Fu SN, Effects of habitual loading on patellar tendon mechanical and morphological properties in basketball and volleyball players: Eur J Appl Physiol, 2015; 115; 2263-69
20. Huang JP, Qin K, Tang CZ, Assessment of passive stiffness of medial and lateral heads of gastrocnemius muscle, achilles tendon, and plantar fascia at different ankle and knee positions using the MyotonPRO: Med Sci Monit, 2018; 24; 7570-76
21. Haen TX, Roux A, Soubeyrand M, Shear waves elastography for assessment of human Achilles tendon’s biomechanical properties: An experimental study: J Mech Behav Biomed, 2017; 69; 178-84
22. Konor MM, Morton S, Eckerson JM, Grindstaff TL, Reliability of three measures of ankle dorsiflexion range of motion: Int J Sports Phys Ther, 2012; 7; 279-87
23. Sackley C, Physical therapy research – principles and applications: Physiotherapy, 1993; 79; 612
24. Ko CY, Choi HJ, Ryu J, etween-day reliability of MyotonPRO for the non-invasive measurement of muscle material properties in the lower extremities of patients with a chronic spinal cord injury: J Biomech, 2018; 73; 60-65
25. Jeon M, Youn K, Yang S, Reliability and quantification of gastrocnemius elasticity at relaxing and at submaximal contracted condition: Med Ultrason, 2018; 20; 342-47
26. Saeki J, Ikezoe T, Nakamura M, The reliability of shear elastic modulus measurement of the ankle plantar flexion muscles is higher at dorsiflexed position of the ankle: J Foot Ankle Res, 2017; 10; 18
27. Taş S, Salkın Y, An investigation of the sex-related differences in the stiffness of the Achilles tendon and gastrocnemius muscle: Inter-observer reliability and inter-day repeatability and the effect of ankle joint motion: Foot (Edinb), 2019; 41; 44-50
28. Ludbrook J, Confidence in Altman-Bland plots: A critical review of the method of differences: Clin Exp Pharmacol Physiol, 2010; 37; 143-49
29. Shan X, Otsuka S, Yakura T, Morphological and mechanical properties of the human triceps surae aponeuroses taken from elderly cadavers: implications for muscle-tendon interactions: PLoS One, 2019; 14(2); e021148
30. MaiSetti O, Hug F, Bouillard K, Characterization of passive elastic properties of the human medial gastrocnemius muscle belly using supersonic shear imaging: J Biomech, 2012; 45; 978-84
31. DeWall RJ, Slane LC, Lee KS, Spatial variations in Achilles tendon shear wave speed: J Biomech, 2014; 47; 2685-92
32. Zhou J, Liu C, Zhang Z, Non-uniform stiffness within gastrocnemius-Achilles tendon complex observed after static stretching: J Sports Sci Med, 2019; 18; 454-61
33. Sébastien A, Risson JR, Adrian K: Skeletal Radiol, 2013; 42; 1143-50
34. Arndt A, Bengtsson AS, Peolsson M, Non-uniform displacement within the Achilles tendon during passive ankle joint motion: Knee Surg Sports Traumatol Arthrosc, 2012; 20; 1868-74
35. Slane LC, Thelen DG, Non-uniform displacements within the Achilles tendon observed during passive and eccentric loading: J Biomech, 2014; 47; 2831-35
36. Arampatzis A, Stafilidis S, Demonte G, Strain and elongation of the human gastrocnemius tendon and aponeurosis during maximal plantarflexion effort: J Biomech, 2005; 38; 833-41
37. Finni T, Hodgson JA, Lai AM: J Appl Physiol, 2003; 95; 829-37
38. Handsfield GG, Inouye JM, Slane LC, A 3D model of the Achilles tendon to determine the mechanisms underlying nonuniform tendon displacements: J Biomech, 2017; 51; 17-25
39. Slane LC, Thelen DG, Achilles tendon displacement patterns during passive stretch and eccentric loading are altered in middle-aged adults: Med Eng Phys, 2015; 37; 712-16
40. Helfenstein-Didier C, Andrade RJ, Brum J: Phys Med Biol, 2016; 61; 2485-96
41. Reeves D, Cooper G, Is human Achilles tendon deformation greater in regions where cross-sectional area is smaller?: J Exp Biol, 2017; 220; 1634-42
42. Iwanuma S, Akagi R, Kurihara T, Longitudinal and transverse deformation of human achilles tendon induced by isometric plantar flexion at different intensities: J Appl Physiol, 2011; 110; 1615-21
43. Coombes BK, Tucker K, Vicenzino B, Achilles and patellar tendinopathy display opposite changes in elastic properties: A shear wave elastography study: Scand J Med Sci Sports, 2018(3); 1201-8
44. Slane LC, Martin J, Dewall R, Quantitative ultrasound mapping of regional variations in shear wave speeds of the aging Achilles tendon: Eur Radiol, 2017; 27; 474-82
Figures
Figure 1. Photograph of the splint.Figure 2. Bland-Altman plots of intra- and inter-rater reliability of Achilles tendon stiffness. (A, B) Intra- and inter-rater reliability of AT-0 stiffness at ankle neutral position. (C, D) Intra and inter-rater reliability of AT-6 stiffness at ankle neutral position. (E, F) Intra- and inter-rater reliability of AT-0 stiffness at ankle dorsiflexion 10°. (G, H) Intra- and inter-rater reliability of AT-6 stiffness at ankle dorsiflexion 10°.Figure 3. The mean stiffness of AT-0 and AT-6 at ankle joint 0° (deep blue) and dorsiflexion 10° (light blue). The difference between AT-0 and AT-6 mean stiffness at 0° and dorsiflexion 10°. *** P<0.001. Tables
Table 1. Inter-and intra-operator reliability of Achilles tendon at the neutral ankle neutral. ICC, intraclass correlation coefficients; CI, confidence interval; SEM (N/m), the standard error of measurement; MDC (N/m), the minimal detectable change; A1B, inter-rater reliability; A1A2, intra-rater reliability.Table 2. Inter-and intra-operator reliability of Achilles tendon at the ankle 10° dorsiflexion. ICC, intraclass correlation coefficients; CI, confidence interval; SEM(N/m), the standard error of measurement; MDC(N/m), the minimal detectable change; A1B, inter-rater reliability; A1A2, intra-rater reliability.Table 1. Inter-and intra-operator reliability of Achilles tendon at the neutral ankle neutral. ICC, intraclass correlation coefficients; CI, confidence interval; SEM (N/m), the standard error of measurement; MDC (N/m), the minimal detectable change; A1B, inter-rater reliability; A1A2, intra-rater reliability.Table 2. Inter-and intra-operator reliability of Achilles tendon at the ankle 10° dorsiflexion. ICC, intraclass correlation coefficients; CI, confidence interval; SEM(N/m), the standard error of measurement; MDC(N/m), the minimal detectable change; A1B, inter-rater reliability; A1A2, intra-rater reliability. In Press
Clinical Research
Effect of Dexmedetomidine Hydrochloride Nasal Spray on Anxiety and Sleep in Patients Undergoing Gynecologic...Med Sci Monit In Press; DOI: 10.12659/MSM.952465
Clinical Research
Prognostic Value of Mortality Scoring Systems in Patients With Severe Burns: Identifying Key Predictors of ...Med Sci Monit In Press; DOI: 10.12659/MSM.951713
Laboratory Research
Evaluation of the Trueness and Precision of Cast, Milled-Cast, Milled, and 3D-Printed Post-and-Core Techniq...Med Sci Monit In Press; DOI: 10.12659/MSM.953491
Clinical Research
Outcomes After Minimally Invasive Intramedullary Nail Fixation and Locking Plate Fixation Among Patients Wi...Med Sci Monit In Press; DOI: 10.12659/MSM.952670
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,214
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,757,839
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,153
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,809
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387