04 January 2023: Clinical Research
The Effects of Offering Freedom to Comply by Pediatricians and Nurses, Using the But-You-Are-Free (BYAF) Technique, on Vaccination Compliance on 185 Parents of Newborn Babies Conducted in Outpatient Clinics in Poland Between January 2022 and July 2022
Dariusz DolińskiDOI: 10.12659/MSM.938743
Med Sci Monit 2023; 29:e938743






Abstract
BACKGROUND: This study aimed to evaluate, in outpatient clinics in Poland between January 2022 and July 2022, the effectiveness of the But-You-Are-Free (BYAF) social influence technique by healthcare professionals during interaction with 185 parents deciding about vaccinating (eg, Hexacima, Prevenor 13, Synflorix, Rotateq, Act Hib, Boostrix, Pentaxim, DTP, Imovax, Priorix, MMR, Tetracim, Adacel, Euvax B, Fuvax, FSME, Varilix, Nimenrix, Bexero vaccines) their babies.
MATERIAL AND METHODS: During an interaction with pediatricians or nurses, the parents were encouraged to vaccinate their babies. In experimental condition (111 interactions), the BYAF technique was employed, and the phrase “But you are free” was added at the end of the conversation. In the control condition (74 interactions), it was not employed.
RESULTS: In the experimental condition, 71 (64%) participants declared intention to vaccinate their children. In the control condition, it 61 (84%) participants declared intention to vaccinate (the difference in percentages was significant: P=0.006). The number of parents who actually vaccinated their babies in the experimental condition was 92 (83%) and in the control condition it was 70 (95%; P=0.018).
CONCLUSIONS: The findings showed that participants who were exposed to the BYAF technique declared lower intentions to vaccinate their babies, and vaccinated them less often than those in the control condition. This result critically highlights that this technique should not be employed in the medical settings of pediatric vaccination.
Keywords: Immunization Programs, Mass Vaccination, Vaccination, Vaccination Refusal, Infant, Infant, Newborn, Humans, Child, Poland, Parents, Pediatricians, Ambulatory Care Facilities, Freedom, Health Knowledge, Attitudes, Practice
Background
“BUT YOU ARE FREE” TECHNIQUE:
The need for autonomy and freedom is one of the most powerful and universal human psychological needs. According to classic reactance theory [7], perceived threat to personal freedom creates a strong aversive state which motivates people to find different ways to reestablish their freedom. People who are asked by someone (especially a stranger) to do something may not feel completely free. A possible decision to fulfill a request has its origin not in their mind, but in an external factor (ie, in another person’s request). The requested person therefore does not feel like someone who freely made a decision about a certain behavior on their own. On the contrary, it was someone else who made them do it.
The “but you are free” (BYAF) technique, which was founded on the notion that the compliance rate might be increased by including in the request a convincing evocation of the freedom punchline, is effective because it restores a sense of agency [7]. In other words, this technique is very promising due to eradicating obstacles while persuading somebody to perform specific actions. A person who is told ”but the choice is yours”, ”but you are free to accept or refuse”, or ”but obviously do not feel obliged” feels like the originator of their action and, paradoxically, as research shows, complies with the request.
In numerous studies it has been demonstrated that, as predicted by the aforementioned reactance theory, the BYAF technique consistently increases compliance with a variety of requests, such as completing a survey [8–11], donating money to a non-profit organization [6,11], allowing a stranger to borrow a mobile phone to make a call [8,12], or obtaining some monetary change from a stranger to take the bus [6]. According to results of a meta-analysis, this simple technique is robust, highly reliable, and effective. Ending a request with a phrase recognizing the target’s freedom to say ”no” more or less doubles the chances of fulfilling the request [13]. Importantly, to date, this technique was never tested in the medical environment.
The aim of our research was to test the effectiveness of the BYAF technique in an unresearched area of application – encouraging parents to vaccinate their children. In many third-world countries, the main reason for the low percentage of vaccinated children is the low availability and/or high cost of vaccines [14]. Fortunately, this situation is gradually changing and after almost every passing year, more and more of the world’s population is gaining access to vaccination [15,16]. At the same time, however, one may observe a decline in childhood immunization in countries where vaccinating is broadly available and often even free [17–19]. Due to various fake news pieces appearing on the Internet, parents who are falsely convinced that vaccines can be harmful are refusing to vaccinate their children [19,20]. Relatively often, their decision is preceded by a conversation with a doctor, midwife, nurse, or other healthcare professional, who obviously use various arguments to encourage parents to vaccinate their offspring [20]. However, these discussions do not always result in parents making the desired decision.
Therefore, this study aimed to evaluate the effects of offering freedom to comply by pediatricians and nurses, using the But-You-Are-Free (BYAF) technique, on vaccination compliance on 185 parents of newborn babies conducted in outpatient clinics in Poland between January 2022 and July 2022.
Material and Methods
ETHICS STATEMENT:
The study was approved by Ethics Commitee for Human Research of SWPS University, Wrocław Faculty (no. 09/P/02/2021).
STUDY DESIGN:
As aforementioned, the effectiveness of the BYAF technique has been confirmed in numerous studies [6,8–12]. However, it was never been tested in the healthcare area. Thus, the current study was the first one in this field. Its purpose was to examine the effectiveness of the BYAF technique in the environment of the mass immunization of infants and children. During the visits of parents with their children in an outpatient clinic, pediatricians and nurses (in experimental condition) encouraged them to vaccinate their babies but at the same time they offered to some of the parents freedom to comply using the BYAF technique: they indicated that the decision to vaccinate the babies belongs to the parents by adding the phrase: “but you are free”.
The study had an experimental design. There were 2 dependent variables: intention of vaccinating the baby and actual vaccination. This research was not aimed to test the BYAF technique in relation to a specific vaccine. Our purpose was to test the effectiveness of the BYAF technique in encouraging parents to vaccinate their children in general. Since vaccination took place in an outpatient clinic, children were of different ages, many types of the vaccines were used in this study, including Hexacima, Prevenor 13, Synflorix, Rotateq, Act Hib, Boostrix, Pentaxim, DTP, Imovax, Priorix, MMR, Tetracim, Adacel, Euvax B, Fuvax, FSME, Varilix, Nimenrix, and Bexerol. The aim of this study was to assess actions and attitudes towards vaccines in general, and not to test the BYAF technique regarding a specific vaccine and/or maker of the vaccine.
PARTICIPANTS:
We included 185 parents (168 mothers and 17 fathers) in this study. The participants were Polish, aged 19 to 48 years. All of them were patients of clinics for children but they needed to see a doctor due to reasons other than vaccination (eg, baby’s infection or routine examination).
DATA COLLECTION AND EXPERIMENTAL MANIPULATION:
The study was conducted from January 2022 to July 2022 in clinics for children. The data of participants, like gender, age, and education, were gathered by the doctors or nurses. The participants were also asked about the course and possible complications of their pregnancy and childbirth. If the child was not their first, the parents answered the question of whether their previous children had been vaccinated. During an interaction with pediatricians or nurses, all the participants were encouraged to vaccinate their children and informed about the effectiveness, importance, and possible adverse effects of the vaccines. However, in 111 cases (experimental condition), at the end of the conversation the doctor or nurse offered the parents freedom to comply by using the phrase: “but you are free” (to vaccinate your baby or not). The other 74 participants were not told that (control condition). This method was based on the literature on the BYAF technique [6,8–12]. Next, the participants had to answer the question of whether they had decided to vaccinate their baby. All of them were thanked for their participation in the study. Finally, we received information (from the doctors) on whether the baby was eventually vaccinated or not.
STATISTICAL ANALYSIS:
The data were collected in Excel and then manually verified by the investigators. SPSS 27.0 Windows software (IMB Corp.) was used for statistical analysis. The main aim of this research was to assess whether the BYAF technique can influence parents’ intentions to vaccinate their children, as well as their actual behavior (ie, vaccinating). In order to answer that question, we determined whether the proportions of participants who intended to vaccinate their children and actually vaccinated them differed between 2 experimental conditions, with the use of the Wald H0 test for independent samples. The statistical data described the number of cases and percentage. The reported Wald Z statistic shows the variance estimates under H0. According to commonly accepted practice, a
Results
GENERAL ANALYZES:
In general, 132 participants (71.4%) declared that they decided to vaccinate their babies. Forty-four (23%) of all participants remained hesitant and 9 (4.9%) of them decided not to vaccinate their babies. Finally, 162 babies (87.6%) have been vaccinated. However, there were some differences between the experimental and the control condition, as can be seen below.
INTENTIONS OF VACCINATING:
In the experimental condition, 71 of 111 parents (64%) and 61 of 74 participants (82.4%) in the control condition declared that they would vaccinate their babies. In the experimental condition, 33 (29.7%) remained hesitant and 7 (6%) participants did not want to vaccinate their babies. In the control condition, there were 11 (14.9%) hesitant participants and 2 (2.7%) who declared that they would not vaccinate their babies. The Wald H0 test indicated that the proportion’s difference between the conditions was significant (Z=2.722;
THE ACTUAL BEHAVIOR (PERCENTAGE OF VACCINATED BABIES):
There were 92 (82.9%) vaccinated babies in the experimental group and 70 (96.4%) in the control group. Once again, the Wald H0 test of proportion indicated that this difference was statistically significant (Z=2.365,
ANALYSIS FOR MANDATORY AND RECOMMENDED VACCINES:
To examine whether the intention to vaccinate after the experimental manipulation depends on the type of vaccine, separate analyses for mandatory and nonmandatory/recommended vaccines were conducted. A total of 134 conversations between healthcare professionals and parents were related to mandatory vaccines (81 of which were in the experimental group, and 53 in the control group). Fifty-one interactions concerned recommended vaccines (30 in the experimental group and 21 in the control group).
INTENTIONS OF VACCINATING:
The analysis for mandatory vaccines showed that the percentage of participants who decided to vaccinate their babies was higher in the control group. The Wald test showed that the difference of proportions between the groups was significant (Z=2.364, P=0.018). The same test showed no significant difference between groups for the recommended vaccines. However, the percentages in both groups were very similar to those for the mandatory vaccines (for numbers and percentages, see Table 1). Thus, the lack of significance was probably caused by the small sample size.
ACTUAL VACCINATING:
Regarding the percentages of babies who have actually been vaccinated with mandatory vaccines, the percentage in the control group was still significantly higher than in the experimental group (Z=2.903; P=0.004). However, the Wald H0 test for recommended vaccines showed no significant differences and the proportions were very similar in both groups (for numbers and percentages, see Table 2).
ANALYZES FOR SINGLE AND COMBINED VACCINES:
Although it was not the main goal of the study, we also decided to conduct separate analyzes for single and combination vaccines. It turned out, however, that the division into categories here is not dichotomous, because some of the conversations between healthcare professionals and parents concerned either several vaccines, some of which belonged to single and some to combined ones, or there was no precise definition of which type of vaccine was meant. Therefore, a separate category “unclassified” was created for vaccines whose type could not be determined. Then, the analysis of intentions and of the actual level of vaccination was performed, distinguishing between these 3 categories.
A total of 89 conversations concerned single vaccines (58 of which were in the experimental group, 31 in the control group), 59 were related to combined vaccines (26 in the experimental group and 33 in the control group), and 37 were unclassified (27 in the experimental group and 10 in the control group).
INTENTIONS OF VACCINATING:
The Wald H0 test showed no significant differences in the percentage of declarations of willingness to vaccine children between the experimental and control groups for both single and combined vaccines. However, for unclassified vaccines, such a difference appeared: Z=2.13; P=0.034. In the experimental condition, parents less frequently declared their willingness to vaccinate their children (numbers and percentages for all 3 categories are shown in Table 3).
ACTUAL VACCINATION LEVEL:
For single vaccines, the percentages of parents who finally vaccinated their children did not differ significantly between groups. However, such differences appeared both in the case of combined (Z=2.33; P=0.020) and unclassified vaccines (Z=2.25; P=0.024). In both cases, the parents in the experimental group vaccinated their children less frequently than those in the control group (numbers and percentages are shown in Table 4).
ANALYSES FOR INDIVIDUAL VACCINES:
As mentioned above, our study did not concern specific vaccines, but rather the majority of childhood vaccines available in Poland. Due to the small sample sizes, statistical analyses did not show differences between groups for any particular vaccine. We created tables showing how many people wanted to talk about vaccines against specific bacteria or viruses, how many of them in each group declared that they wanted their child vaccinated, and how many of them actually vaccinated the child. The numbers for the single vaccines are presented in Table 5 and for the combination vaccines in Table 6. The most doubts among the parents were raised by the combination vaccines against measles, mumps, and rubella (MMR and Priorix).
Discussion
The use of the BYAF social influence technique while persuading parents to vaccinate their children reduced, contrary to existing literature on this phenomenon, their consent to vaccination with both the mandatory and nonmandatory/recommended vaccines. The counterproductive effect of this technique was also observed in relation to the mere fact of coming to the doctor’s office for the mandatory immunization. In the case of the recommended vaccination, there were no differences between the condition in which the BYAF technique (experimental group) was used and the control condition in which it was not used (control group). The use of BYAF technique has also decreased the parents’ compliance to vaccination with combined vaccines, but not for single vaccines.
Without exception all scientific articles published so far in the field of social influence demonstrated a very high effectiveness of the BYAF technique in gaining compliance. Our study is the first empirical study in medical settings to show that the BYAF technique is not effective and that its use reduces patients’ compliance. In short, it backfires by reducing vaccination. One should, however, consider that the technique has so far been shown to be effective in dealing with rather trivial requests, like completing a survey [8–10], donating money for charity [6,11], allowing another person to borrow a mobile phone to make a call [9,12], or giving money to strangers to take a bus [6]. On the contrary, the decision to vaccinate or not vaccinate a child is definitely not a trivial one and this may be a key factor in explaining the pattern of results we found, and this very difference may explain the unexpected pattern of results reported in our study.
It is unclear why the pattern of results is exactly opposite, not only to the theoretical rationale of the theory of reactance described in the introduction, but also to the body of research on this social influence technique supported by a meta-analysis proving the robustness of the effect [13]. It is possible that in the case of the decision making when a doctor or other healthcare professional says “but you are free to decide”, this person is simultaneously signaling that they are discarding the responsibility for potential medical consequences, placing that responsibility on the parent, and/or increasing the feeling of the danger (“since this person is stepping down from the responsibility, this decision has to be very risky”).
Alternatively, perhaps under conditions where patients hear ”but the choice is yours”, they may conclude that the best option (vaccination vs refusal to vaccinate) is not clear-cut. If you have to make a decision, it means that the substance is unclear, and calls for deliberation. Obligatory decisions without a choice are clear and safe (we pay taxes, vaccinate, keep to the right side of the traffic while driving, and we do not hear questions about the choice). So, apparently, such communication creates a feeling that there are reasons for both decisions: to vaccinate and not to vaccinate. Since leaving room for such deliberation while deciding on non-mandatory/non-obligatory vaccines is natural, in the case of mandatory vaccines, such room for choice may create opposite tendencies of vaccine hesitancy.
It is worth stressing that in both the above-mentioned hypothetical situations (ie, both when a doctor is seen as a person who does not want to take responsibility for the possible negative consequences of vaccination, and when the patient has a feeling that the choice is not obvious because both options have some advantages and disadvantages), one can expect that some people would decide not to vaccinate their children.
The result that in the case of recommended vaccination the use of the BYAF technique reduced parents’ consent to immunization during a conversation with medical staff, but at the same time did not reduce their tendency to actually vaccinate their child a bit later, calls for additional in-depth explanation.
Social psychology provides a large amount of empirical evidence showing that verbal statements about one’s attitudes, decisions, and behaviors may even be, in particular situations, completely different from actual behavior [21,22], and this explain the pattern we found. There is, however, an open question of why it happened in this study. The parents interact about health-related issues outside the clinic (with family and friends), during which their social circle may effectively encourage them to change their opinion and, as a consequence, to immunize the child.
The study also indicated that the differences between the parents who have been offered freedom to comply by using the BYAF technique and those who have not was related to combined vaccines, not to single ones. A possible explanation is that parents usually have more concerns about combined vaccines, for example a fear of immune overload [23] or complications like autism [20]. It is possible that these concerns increase vaccination hesitancy or vaccination refusal, especially when combined with using the BYAF technique.
Sadly, and contrary to the research presented above, the vast majority of research conducted in the field of social sciences does not study the real behavior of people, but only their verbal declarations about hypothetical situations [24]. The study presented above fills this important gap: we asked people in a real (not hypothetical) situation if they intended to immunize their child, and subsequently determined if they actually did so.
The second clear advantage of our research was that it was conducted in different locations ruling out the possibility that one specific location or one doctor or nurse was responsible for the pattern of results, which would make replications/applications impossible. In this way our research clearly delivers the robustness of the effect and the generalizability of the results.
Thirdly, we have tested the effectiveness of this technique not only on obligatory vaccines but also recommended vaccines, showing a wider perspective for application. Despite the fact that the pattern of results we obtained turned out to be completely surprising, it indicates that medical staff should not use phrases like “but the choice is yours” or “but it is you who have to make a decision” in conversations about vaccinations with patients. Keeping this in mind, our research addressed both lines of everyday interactions of healthcare professionals and parents.
Of course, our study has clear limitations. Firstly, since it was run in the context of a clinic for children, our results do not allow conclusions about vaccinations in general. We do not know if the same pattern of results would be obtained while researching vaccinations for adults who are not only the decision makers but also the targets of those decisions.
Secondly, a particularly important limitation of this study is that many different types of vaccines were considered (eg, Hexacima, Prevenor 13, Synflorix, Rotateq, Act Hib, Boostrix, Pentaxim, DTP, Imovax, Priorix, MMR, Tetracim, Adacel, Euvax B, Fuvax, FSME, Varilix, Nimenrix, and Bexero). Additionally, some vaccines were provided combined with others, which expanded the list of possible combinations for analysis by reducing the number of participants per experimental condition to critically low values (eg, sample size for WZW B vaccine;
Thirdly, since it was conducted in a single country (albeit in many locations) it is still possible that these results are restricted solely to this region of the world.
Usually in such situations, the authors declare that further replication studies of the problem are necessary. In this particular case, however, there is a serious ethical problem. When proceeding with our research, we asked ourselves whether the BYAF social influence technique would also be effective in persuading people to vaccinate. The clear pattern of results obtained by us, indicating its counter-effectiveness in encouraging people to vaccinate, was completely surprising. We discuss the phenomenon of BYAF with regard to the burden and fear of taking responsibility for decisions concerning the vaccination of one’s own child. At the same time, fear and responsibility by itself may not be the main modulator, while the same effect has not worked out in agreement with the examination, treatment, and medical interventions in other areas of hospital procedures and non-infectious medicine. This means that there are probably some other modulators, such as fear of social judgment, fear of skeptics, fear of potential complications, and finally the influence of the media and anti-vaccine marketing. The identification of such factors/modulators can be important for prophylaxis and health promotion effects, with the widespread availability of vaccines. Conducting further research on this technique in the natural setting would very likely discourage some people from vaccination, which would further facilitate vaccine hesitancy, especially during the global COVID-19 pandemic. Therefore, we will not conduct further research on this paradigm.
Conclusions
This paper reports the first study on the BYAF social influence technique applied in medical settings. The results are contrary to what was expected and previously reported in the literature on that issue: participants in the control group declared higher intentions to vaccinate their babies, and actually vaccinated them more often, than those in the experimental group. This result critically highlights the techniques that should not be employed in the medical setting of pediatric vaccination.
We may conclude that it is very likely that in such a situation the child’s parents do not want to hear that the choice is theirs, because it makes them confused. The situation is unclear and ambiguous. It is better if the doctor or midwife simply advises parents that their child should be immunized without providing a choice.
Tables
Table 1. Intentions to vaccinate babies.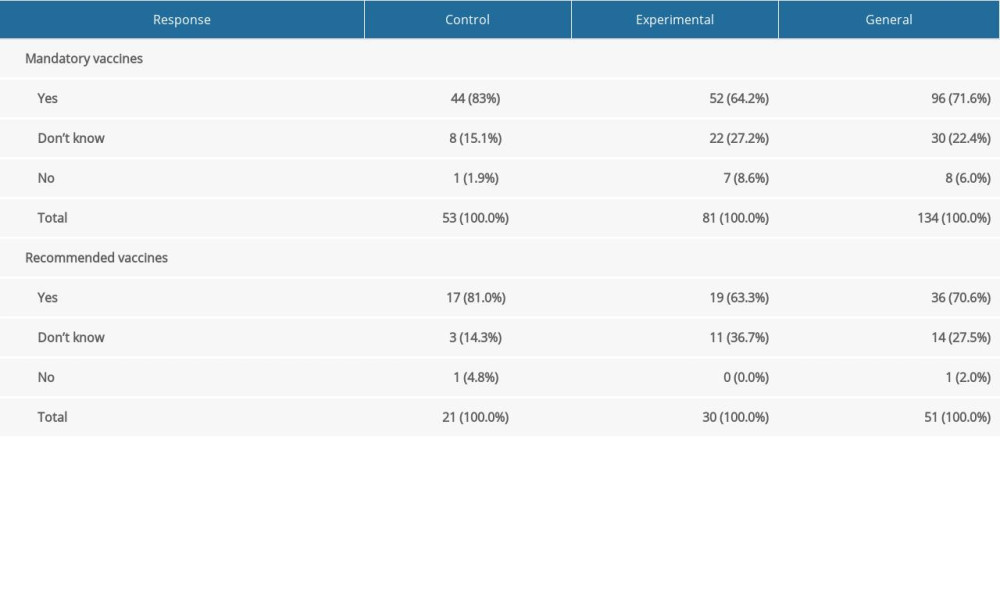 Table 2. Numbers and percentages of babies who really have/have not been vaccinated.
Table 2. Numbers and percentages of babies who really have/have not been vaccinated.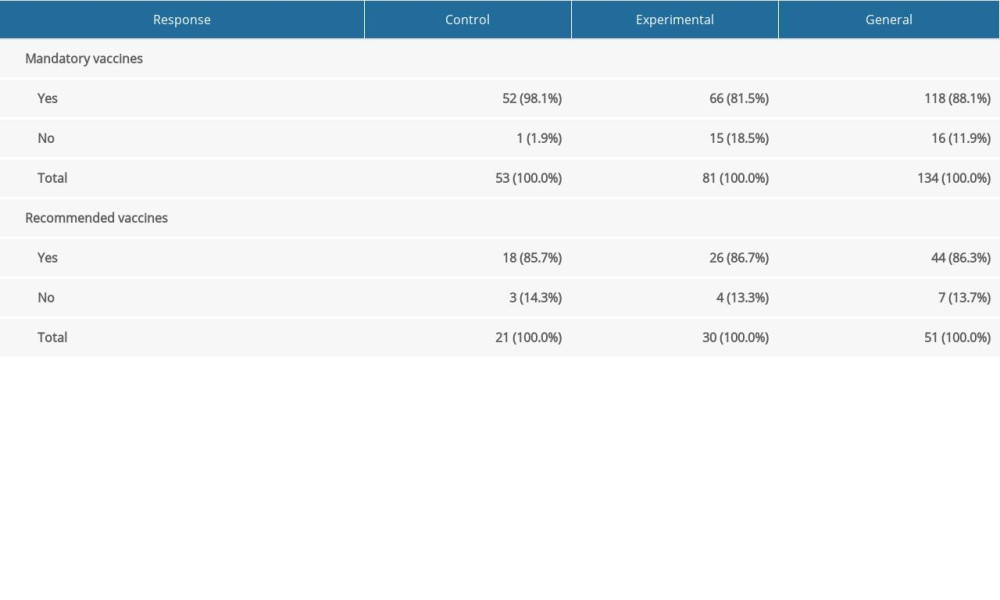 Table 3. Intentions of babies’ vaccination for single, combined and not classified vaccines.
Table 3. Intentions of babies’ vaccination for single, combined and not classified vaccines.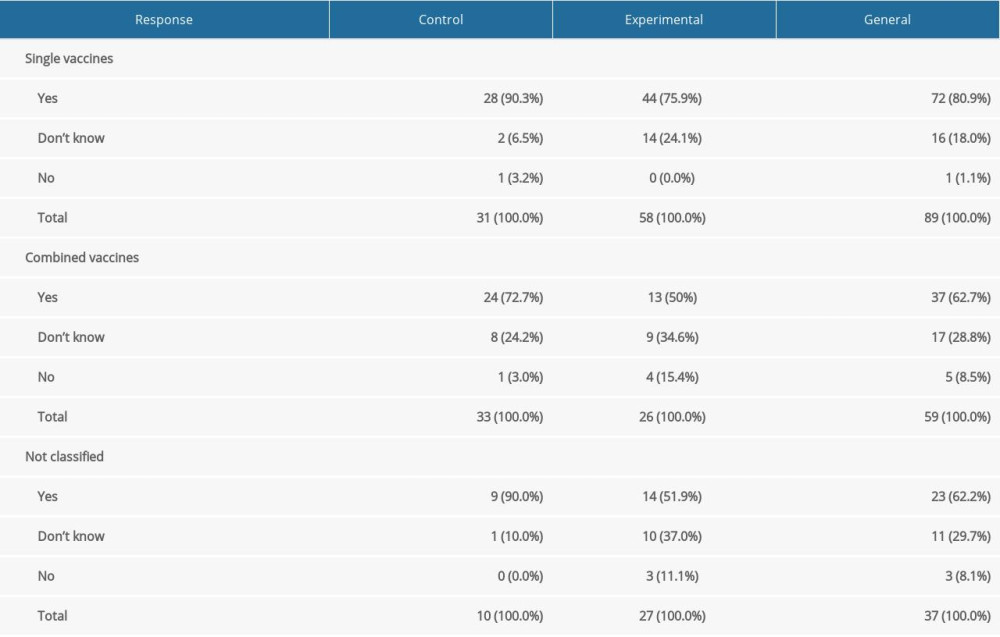 Table 4. Numbers and percentages of children who really have/not been vaccinated for single, combined and not classified vaccines.
Table 4. Numbers and percentages of children who really have/not been vaccinated for single, combined and not classified vaccines.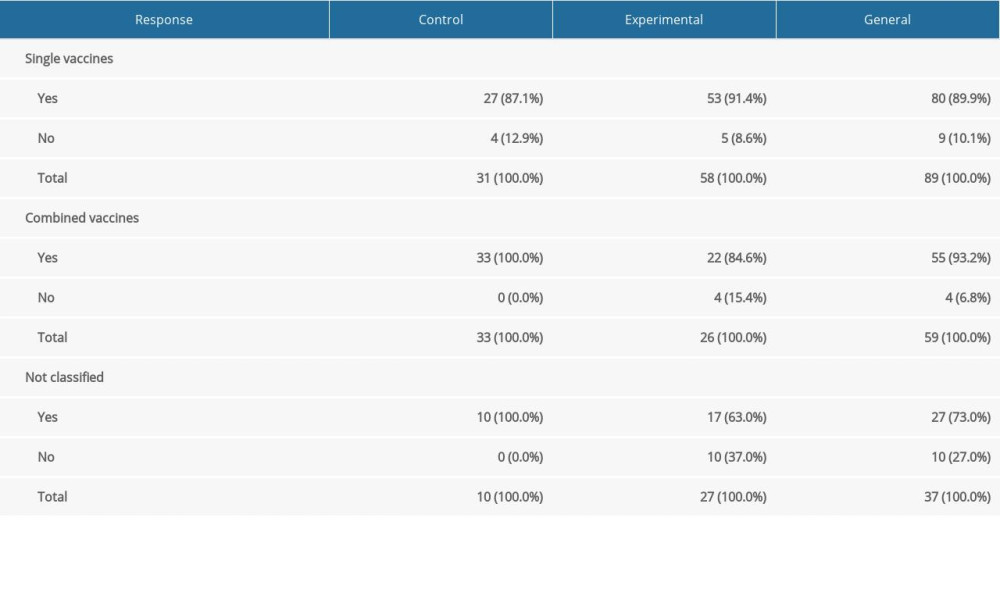 Table 5. Declarations and vaccinations for single vaccines.
Table 5. Declarations and vaccinations for single vaccines.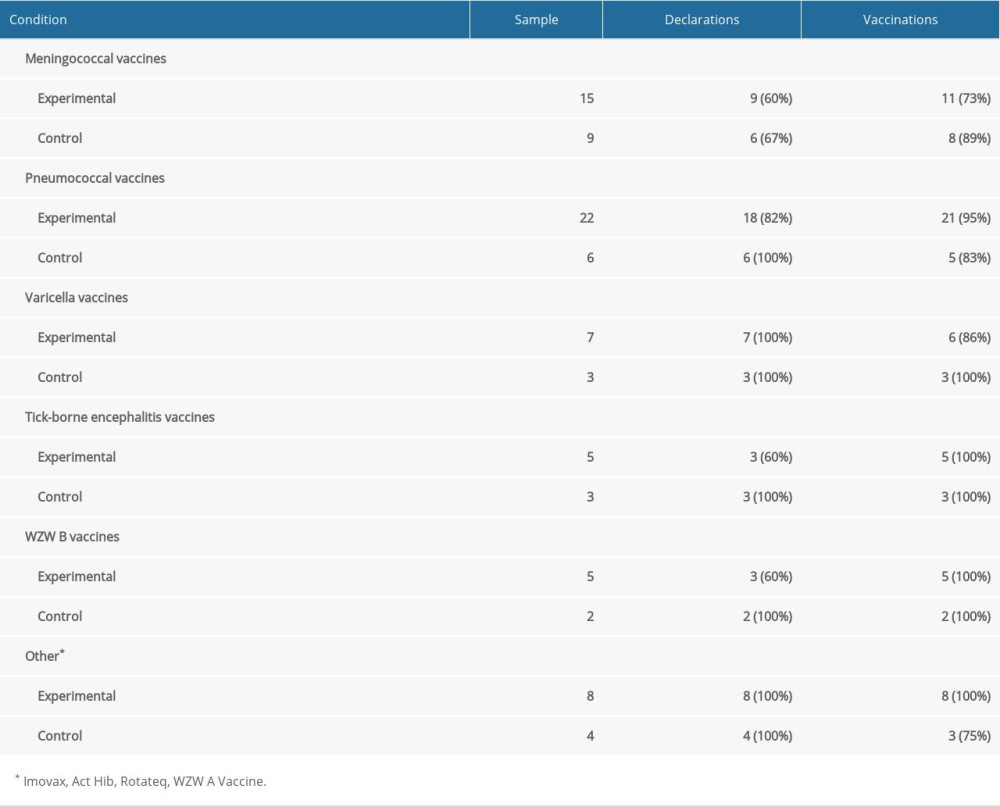 Table 6. Declarations and vaccinations for combined vaccines.
Table 6. Declarations and vaccinations for combined vaccines.
References
1. Shuai W, Bingfeng H, Yongmei W, Do male university students know enough about human papillomavirus (HPV) to make informed decisions about vaccination?: Med Sci Monit, 2020; 26; e924840
2. Cialdini RB, Influence: The psychology of persuasion, 2021, New York, HarperCollins
3. Dolinski D, Techniques of social influence: The psychology of gaining compliance, 2016, London, Routledge
4. Dolinski D, Grzyb T: 100 effective techniques of social influence When and why people comply, 2023, London, Routledge
5. Pratkanis AR: The science of social influence Advances and progress, 2014, Psychology Press
6. Guéguen N, Pascual A, Evocation of freedom and compliance: The „but you are free of…” technique: Curr Res Soc Psychol, 2000; 5; 264-70
7. Brehm JW: A theory of psychological reactance\, 1966, Cambridge (MA), Academic Press
8. Grassini A, Pascual A, Guéguen N, The effect of „evoking freedom” techniques on sales in a computer-mediated field setting: Int Rev Retail Distrib Cons Res, 2012; 22; 435-37
9. Farley SD, Kelly J, Singh S, „Free to say no”: Evoking freedom increased compliance in two field experiments: J Soc Psychol, 2019; 159; 482-89
10. Pascual A, Oteme C, Samson L, Cross-cultural investigation of compliance without pressure: The „you are free to…” technique in France, Ivory Coast, Romania, Russia, and China: Cross Cult Res, 2012; 46; 394-416
11. Meineri S, Dupre M, Guéguen N, Door-in-the-face and but-you-are-free: Testing the effect of combining two no-pressure compliance paradigms: Psychol Rep, 2016; 119; 276-89
12. Guéguen N, Silone F, David M, The effect of the „evoking freedom” technique on an unusual and disturbing request: Psychol Rep, 2015; 116; 936-40
13. Carpenter Ch, A meta-analysis of the effectiveness of the „but you are free” compliance gaining technique: Commun Stud, 2013; 64; 6-17
14. Turner HC, Thwaites GE, Clapham HE, Vaccine-preventable diseases in lower-middle-income countries: Lancet Infect Dis, 2018; 18; 937-39
15. Vanderslot S, Dadonaite B, Roser M: Vaccination: Published online at OurWorldInData.org, 2013 [retrived from: ]https://ourworldindata.org/vaccination
16. Rodrigues CMC, Plotkin SA, Impact of vaccines; Health, economic and social perspectives: Front Microbiol, 2020; 11; 1526
17. Carrillo-Santisteve P, Lopalco PL, Measles still spreads in Europe: Who is responsible for the failure to vaccinate?: Clin Microbiol Infect, 2012; 18; 50-56
18. Lo NC, Hotez PJ, Public health and economic consequences of vaccine hesitancy for measles in the United States: JAMA Pediatr, 2017; 171; 887-92
19. Wilder-Smith AB, Qureshi K, Resurgence of measles in Europe: A systematic review on parental attitudes and beliefs of measles vaccine: J Epidemiol Glob Health, 2020; 10; 46-58
20. Shelby A, Ernst K, Story and science. How providers and parents can utilize storytelling to combat anti-vaccine misinformation: Hum Vaccin Immunother, 2013; 9(8); 1795-801
21. Bechler ChJ, Tormala ZL, Rucker DD, The attitude-behavior relationship revisited: Psychol Sci, 2021; 32(8); 1285-97
22. Glasman LR, Albarracin D, Forming attitudes that predict future behavior: A meta-analysis of the attitude-behavior relation: Psychol Bull, 2006; 123(5); 778-822
23. Hilton S, Petticrew M, Hunt K, ‘Combined vaccines are like a sudden onslaught to the body’s immune system’: Parental concerns about vaccine ‘overload’ and immune-vulnerability’: Vaccine, 2006; 24(20); 4321-27
24. Dolinski D, Is psychology still a science of behaviour?: Soc Psychol Bull, 2018; 13(2); 1-14
Tables
Table 1. Intentions to vaccinate babies.Table 2. Numbers and percentages of babies who really have/have not been vaccinated.Table 3. Intentions of babies’ vaccination for single, combined and not classified vaccines.Table 4. Numbers and percentages of children who really have/not been vaccinated for single, combined and not classified vaccines.Table 5. Declarations and vaccinations for single vaccines.Table 6. Declarations and vaccinations for combined vaccines. In Press
26 Mar 2024 : Clinical Research
New Computerized Planning Algorithm and Clinical Testing of Optimized Nuss Bar Design for Patients with Pec...Med Sci Monit In Press; DOI: 10.12659/MSM.943705
07 May 2024 : Clinical Research
Treatment of AVN-Induced Proximal Pole Scaphoid Nonunion Using a Fifth and Fourth Extensor Compartmental Ar...Med Sci Monit In Press; DOI: 10.12659/MSM.944553
16 Mar 2024 : Clinical Research
Diagnostic Efficiency of ACR-TIRADS Score for Differentiating Benign and Malignant Thyroid Nodules of Vario...Med Sci Monit In Press; DOI: 10.12659/MSM.943228
08 May 2024 : Clinical Research
Effect of Individualized PEEP Guided by Driving Pressure on Diaphragm Function in Patients Undergoing Lapar...Med Sci Monit In Press; DOI: 10.12659/MSM.944022
Most Viewed Current Articles
17 Jan 2024 : Review article
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
14 Dec 2022 : Clinical Research
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387
01 Jan 2022 : Editorial
Editorial: Current Status of Oral Antiviral Drug Treatments for SARS-CoV-2 Infection in Non-Hospitalized Pa...DOI :10.12659/MSM.935952
Med Sci Monit 2022; 28:e935952