10 July 2021: Database Analysis
Outcomes of Targeted Temperature Management for In-Hospital and Out-Of-Hospital Cardiac Arrest: A Matched Case-Control Study Using the National Database of Taiwan Network of Targeted Temperature Management for Cardiac Arrest (TIMECARD) Registry
Yu-san Chien12BCDEF, Min-Shan Tsai3B, Chien-Hua Huang3A, Chih-Hung Lai4AB, Wei-Chun Huang5A, Lung ChanDOI: 10.12659/MSM.931203
Med Sci Monit 2021; 27:e931203






Abstract
BACKGROUND: This study aimed to compare outcomes of targeted temperature management (TTM) for patients with in-hospital and out-of-hospital cardiac arrest using the national database of TaIwan network of targeted temperature ManagEment for CARDiac arrest (TIMECARD) registry.
MATERIAL AND METHODS: A retrospective, matched, case-control study was conducted. Patients with in-hospital cardiac arrest (IHCA) treated with TTM after the return of spontaneous circulation (ROSC) were selected as the case group and controls were defined as the same number of patients with out-of-hospital cardiac arrest (OHCA), matched for sex, age, Charlson comorbidity index, and cerebral performance category. Neurological outcome and survival at hospital discharge were the primary outcome measures.
RESULTS: Data of 103 patients with IHCA and matched controls with OHCA were analyzed. Patients with IHCA were more likely to experience witnessed arrest and bystander cardiopulmonary resuscitation (CPR). The duration from collapse to the beginning of CPR, CPR time, and the duration from ROSC to initiation of TTM were shorter in the IHCA group but their initial arterial blood pressure after ROSC was lower. Overall, 88% of patients survived to completion of TTM and 43% survived to hospital discharge. Hospital survival (42.7% vs 42.7%, P=1.00) and favorable neurological outcome at discharge (19.4% vs 12.7%, P=0.25) did not differ between the 2 groups.
CONCLUSIONS: The findings from the national TIMECARD registry showed that clinical outcomes following TTM for patients with IHCA were not significantly different from OHCA when baseline factors were matched.
Keywords: Hypothermia, Induced, out-of-hospital cardiac arrest, Post-Cardiac Arrest Syndrome, Cardiopulmonary Resuscitation, Case-Control Studies, Databases, Factual, Emergency Medical Services, Hospitals, Patient Discharge, Registries, Taiwan
Background
In-hospital cardiac arrest (IHCA) is a highly morbid event with an incidence of 1.51 to 3.25 events per 1000 admissions reported in the literature [1,2]. Less than 20% of patients who were successfully resuscitated after IHCA survived to discharge [1–3] and half of the survivors died within 1 year [4]. Unlike patients who experienced out-of-hospital cardiac arrest (OHCA), IHCA patients tend to present with more pre-existing comorbidities and higher disease severity at the time of cardiac arrest [5,6]. Around 80% of them had a non-shockable initial rhythm [7,8]. They are also more likely to experience witnessed collapse, bystander cardiopulmonary resuscitation (CPR), and have medical professionals as first responders who have access to tools and medications not readily available to OHCA responders [5,9]. Compared with OHCA, the rate of regain spontaneous circulation (ROSC) among IHCA patients was higher, ranging between 42% and 66% [1–3], and their duration of resuscitation was shorter [10]. Given the aforementioned differences, whether treatments proved to improve outcomes of OHCA would be equally effective in IHCA patients requires more investigation.
Targeted temperature management (TTM) is a complex therapeutic intervention designed to induce and maintain body temperature at mild hypothermia for a certain period of time [11]. TTM exerts its neuroprotective effects through multiple mechanisms, including reduction of brain metabolism, attenuation of reactive oxygen species formation, attenuation of immune response during reperfusion, and blockage of apoptosis. It has been used in critically ill patients, such as post-cardiac arrest survivors, patients with traumatic brain injury, and hypoxic encephalopathy in newborns [11,12], but it has also been linked to complications such as secondary infections, ventilator-associated pneumonia, sepsis, coagulopathy, and electrolytes imbalance, especially in those with pre-existing conditions [13,14]. TTM gradually has become standard of care for post-cardiac arrest patients after 2 landmark studies were published in 2002. Researchers found that when survivors of OHCA whose initial rhythm was shockable (ventricular fibrillation or pulseless ventricular tachycardia) were treated with a targeted temperature of 32–34°C, the active temperature control reduced mortality and increased the rate of favorable neurological outcomes [15,16]. Similar benefits were also demonstrated in subsequent studies focusing on OHCA patients who had non-shockable initial rhythm [7,17,18]. In terms of what temperature should be targeted at, Nielsen et al found that for OHCA survivors who remained unconscious, the clinical outcomes of hypothermia at 33°C was not superior to a target at 36°C [19], while a recent trial published in 2019 including 581 comatose cardiac arrest survivors with non-shockable initial rhythm (27.4% of the patients had IHCA) showed that a moderate hypothermia at 33°C led to a better neurologic outcome at 90 days compared with a normothermia group [20].
Based on currently available evidence, the International Liaison Committee on Resuscitation and the American Heart Association [21,22] suggested considering use of TTM, targeting a constant temperature between 32°C and 36°C, in patients who remain comatose after resuscitation from either OHCA or IHCA with any initial rhythm.
The recommendation remains weak for IHCA survivors due to lack of good-quality evidence. So far, no randomized controlled trial has been published that investigated the effects of TTM on IHCA survivors. A few retrospective observational analyses showed only 2–13% of IHCA patients received TTM after regaining spontaneous circulation (ROSC) [23–25], and of those, only about 40% of them had achieved the targeted temperature [6,23]. Of the 5 studies comparing clinical outcomes of IHCA patients treated with TTM versus usual care, 2 were inconclusive (no benefits identified) [26,27], 1 showed that TTM was associated with a favorable neurologic outcome [25], and the other 2 showed that TTM was associated with a lower likelihood of hospital discharge and a worsened neurologic survival [24,28]. Among them, the largest retrospective study focusing on IHCA patients was published in 2013 [28], using data from the Get With The Guideline-Resuscitation Registry. The results indicated potentially harmful effects of therapeutic hypothermia in INCA survivors. However, only 6% of the 26 183 IHCA patients were treated with TTM, which raised the concern of selection bias, and over 75% of the data regarding body temperature in both groups were missing. The results of this study were not considered powerful enough to change the recommendation in guidelines [29]. On the other hand, when comparing IHCA and OHCA patients treated with TTM, 2 retrospective studies published in 2016 showed no differences in short- and long-term survival rates or neurologic outcomes, indicating the benefits of TTM for both groups might be similar [6,30].
Th e present study was conducted to test the hypothesis that benefits of targeted temperature control for patients with IHCA would be similar to those with OHCA when baseline characteristics and comorbidities are controlled, using the national database of TaIwan network of targeted temperature ManagEment for CARDiac arrest (TIMECARD) registry [31].
Material and Methods
STUDY DESIGN AND PATIENT ENROLLMENT:
This multicenter, retrospective, case-controlled study was conducted in Taiwan using data collected from the TaIwan network of targeted temperature ManagEment for CARDiac arrest (TIMECARD) registry. Ten tertiary medical centers participated in this program. Patients over 20 years of age who experienced cardiac arrest and received TTM after successful resuscitation between January 2014 and August 2019 were enrolled. TTM referred to strict temperature control using different cooling devices to target the core body temperature to between 33°C and 36°C following the return of spontaneous circulation (ROSC) after a cardiac arrest, regardless of initial rhythm. TTM protocols and sedation/analgesics/muscle-relaxant protocols varied from hospital to hospital but were accepted by the national academic societies and adhere to international guidelines. Individual patient-level data, delinked with private information, including baseline features, pre-existing comorbidities, location of cardiac arrest, resuscitation characteristics, TTM settings, and possible related complications, clinical course, and outcomes, were recorded using an online case report system [31]. Neurological outcomes were recorded using Glasgow-Pittsburgh cerebral performance category (CPC) scores. A CPC score of 1 or 2 was considered to indicate a favorable neurological outcome, and a CPC score of 3 to 5 was considered to be a poor neurological outcome [16]. Data from electrophysiology studies, including somatic sensory evoked potential and electroencephalogram, and biomarkers of blood or CSF were not available in this registry. The Charlson comorbidity index (CCI) was used to categorize the burden of comorbidities for each patient [32,33]; the index assigns a weight for each comorbid disease, and the score is the total of assigned weights.
All adult cardiac arrest survivors (aged ≥20 years) treated with TTM in the registry were eligible for the present study. Traumatic cardiac arrest was excluded. Study patients were then selected and classified into 2 groups: the case group included patients who experienced IHCA and the control group included those who experienced OHCA, with a 1: 1 ratio matched for age (within 5 years), sex, Charlson comorbidity index (within 2 points), and pre-arrest CPC score (in the same group of performance; good performance defined as 1 or 2 and bad performance defined as a score ≥3) manually. Clinical course, resuscitation, and TTM-related characteristics and outcomes in cases and controls were compared. A shockable rhythm was defined as pulseless ventricular tachycardia or ventricular fibrillation at the beginning of resuscitation. Neurological outcome and survival at hospital discharge were the primary outcome measures.
STATISTICAL ANALYSIS:
Results are expressed as n (%) for categorical variables. Descriptive statistics were reported as mean±standard deviation (SD) or median and interquartile range for continuous variables. The groups were compared using the
Logistic regression models were used to explore independent risk factors for in-hospital mortality and patients’ neurological outcomes. Univariate analyses were performed separately for each risk factor to ascertain the odds ratio and 95% confidence interval. All biologically plausible variables with
Results
During the study period, a total of 580 adult cardiac arrest survivors treated with TTM were registered in the TIMECARD database and 67 of them with traumatic cardiac arrest were excluded. Data from the remaining 513 cases were retrospectively extracted from the registry. Among them, 103 of the 110 patients with IHCA were selected as the case group and the same number of patients with OHCA, matched for age, sex, pre-arrest CCI, and pre-arrest CPC, were selected as the control group. Seven IHCA survivors were not included due to lack of matched controls. Sixty percent of the IHCA patients were resuscitated in either the emergency department (ED) or intensive care unit (ICU) and 34.0% in the ordinary ward. Other locations where IHCA occurred included the hemodialysis room, cardiac catheterization lab, and out-patient clinic.
Baseline characteristics and pre-existing conditions of patients are shown in Table 1. Half of the patients in both groups had a CCI ≥5 (49.5% vs 50.5%,
Resuscitation-associated parameters and characteristics after ROSC are displayed in Table 2. Patients with IHCA were more likely to experience witnessed collapse (95.2% vs 73.8%,
Table 3 shows the comparison of TTM-related variables and clinical outcomes between patients experiencing IHCA vs those experiencing OHCA. Both groups started temperature control 5 hours after ROSC (4.99±4.38 vs 5.35±3.73,
The results of univariate analysis for predictors of survival to discharge are shown in Table 4A. Pre-arrest CPC, pre-arrest CCI, initial shockable rhythm, CPR duration ≥20 minutes, heart rate and systolic blood pressure at ROSC, and new arrhythmia during TTM were significant in a multivariate logistic regression analysis and the data were well fitted by the model (
Discussion
In this case-control study, we used data from the national TIMECARD registry to compare the clinical outcomes of TTM following in-hospital and out-of-hospital cardiac arrest. After matching baseline characteristics, pre-existing comorbidities, and pre-arrest neurologic performance, we found no significant differences in in-hospital survival and neurologic performance at discharge between IHCA and OHCA survivors, indicating that the benefits of TTM are similar in these 2 groups.
Since current guidelines of post-cardiac arrest care for patients experiencing IHCA are mostly based on study results derived from the OHCA population [22], our findings, in line with 2 similar previous studies [6,10], could be used to support the recommendations that suggest use of TTM following in-hospital cardiac arrest [21,22].
However, there are still notable differences in resuscitation-related variables between our case group and control group despite matching (Table 2). IHCA survivors had a shorter time from collapse to initiation of CPR (no-flow time), more witnessed collapse, more bystander CPR, a shorter CPR duration (low-flow time), and a lower blood pressure immediately after resuscitation. Some of these factors were associated with a better clinical outcome after cardiac arrest, and a recent metanalysis showed that bystander CPR contributed to higher survival following OHCA [34]. Duration of resuscitation in patients with IHCA was associated with 30-day survival among those who had ROSC in a Swedish cohort [35]. In another retrospective survey, CPR duration of <20 minutes was found to be an independent predictor for hospital discharge [1]. In contrast, a lower mean arterial blood pressure and a higher heart rate after ROSC were associated with increased in-hospital mortality and worse neurologic performance at discharge [36]. The detrimental effect of lower initial blood pressure might be compensated for by a better resuscitation profile in IHCA patients, but this correlation needs further research to verify.
A survey in 2016 showed 59% of IHCA occurred in ICUs and those who arrested in the ICU were more likely to have pre-existing hypoperfusion, renal and hepatic insufficiency, metabolic abnormalities, and sepsis [37]. Because hypothermia itself can inhibit the cellular immune response, cause cardiac arrhythmia, decrease cardiac output, and suppress renal and cerebral function, it is reasonable to assume that IHCA survivors might be more susceptible to TTM-related complications and therefore have worse clinical outcomes. Our study showed that the incidence of major complications related to TTM were similar in patients experiencing IHCA and those experiencing OHCA if their baseline conditions were matched (Table 3), but we were unable to determine whether the severity and frequency of each documented complication contributed to patients’ survival or neurologic performance.
Our study has some limitations. First, since this study was conducted using data from the national TIMECARD registry, it was subject to the limitations of any retrospective analysis. Associations between variables could be identified but causal relationship could not be established. Second, a selection bias might have occurred. Patients with expected favorable outcomes were more likely to be treated with TTM to optimize the prognosis. In addition, we do not have data on patients who did not receive TTM. Third, our study measured end-points only at the time of hospital discharge, although long-term functional outcomes may be a more robust measurement of any treatment effect on patients recovering from cardiac arrest. Finally, during the 5-year study period, the intensive care for post-cardiac arrest syndrome might have evolved.
Conclusions
The findings from the national TIMECARD registry showed that clinical outcomes of TTM for patients with in-hospital cardiac arrest were not significantly different from those with out-of-hospital cardiac arrest when baseline factors were matched.
Tables
Table 1. Baseline characteristics and pre-existing comorbidities of patients with IHCA and OHCA receiving targeted temperature. Table 2. Resuscitation-associated parameters and characteristics after return of spontaneous circulation of IHCA and OHCA patients receiving targeted temperature management.
Table 2. Resuscitation-associated parameters and characteristics after return of spontaneous circulation of IHCA and OHCA patients receiving targeted temperature management.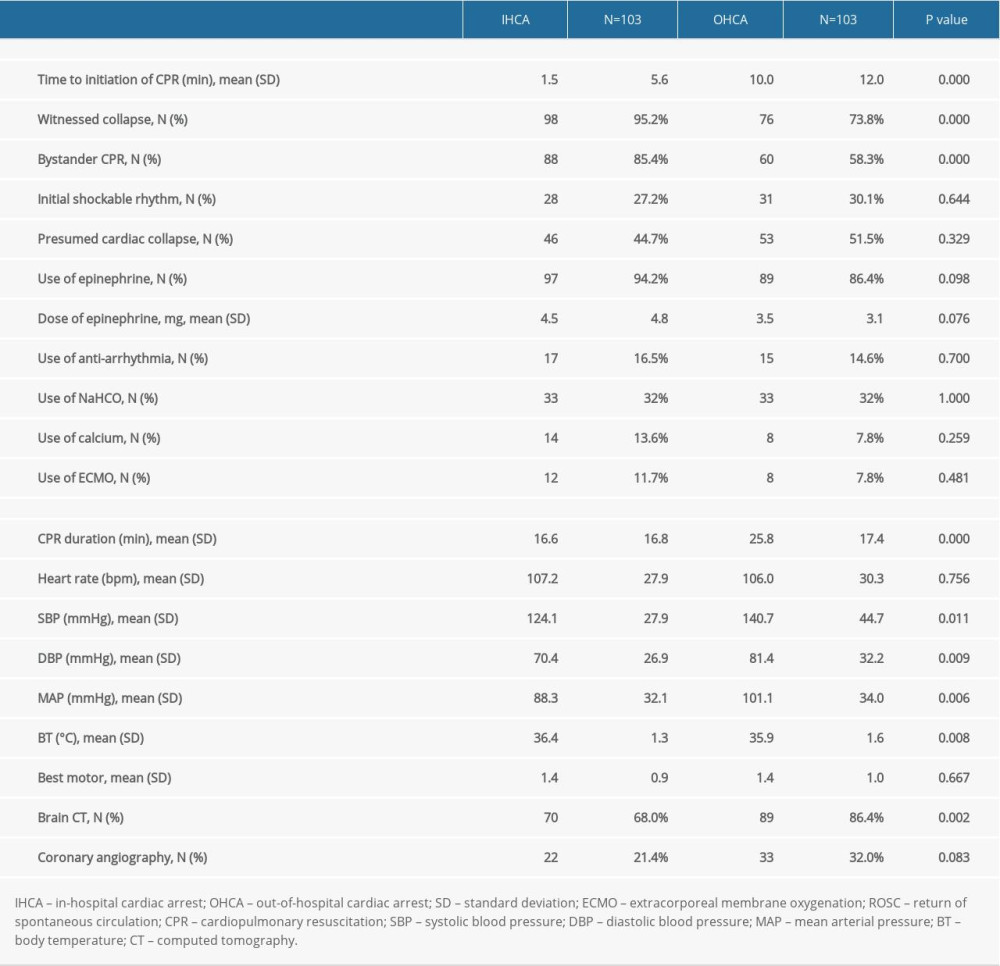 Table 3. Comparison of targeted temperature management related variables and clinical outcomes between patients with IHCA and OHCA.
Table 3. Comparison of targeted temperature management related variables and clinical outcomes between patients with IHCA and OHCA.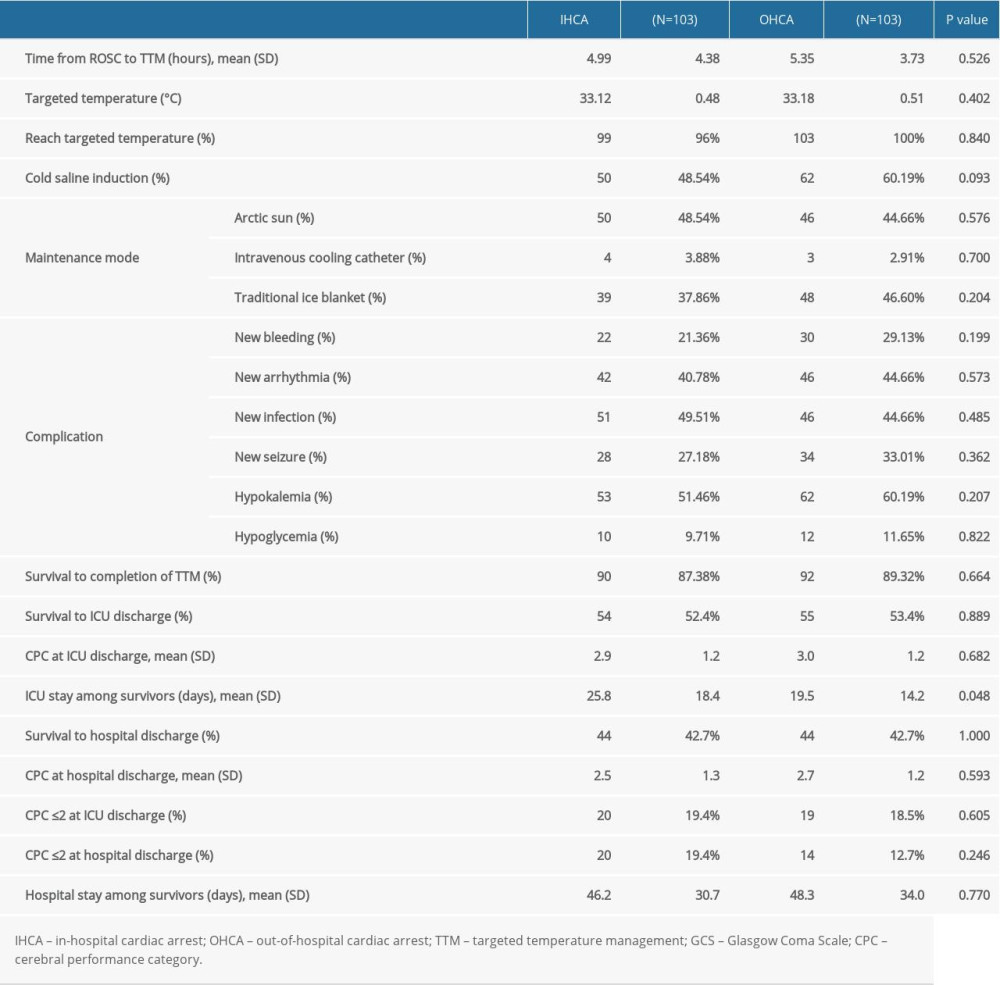 Table 4A. Predictors of survival to hospital discharge among patients receiving targeted temperature control in this cohort.
Table 4A. Predictors of survival to hospital discharge among patients receiving targeted temperature control in this cohort.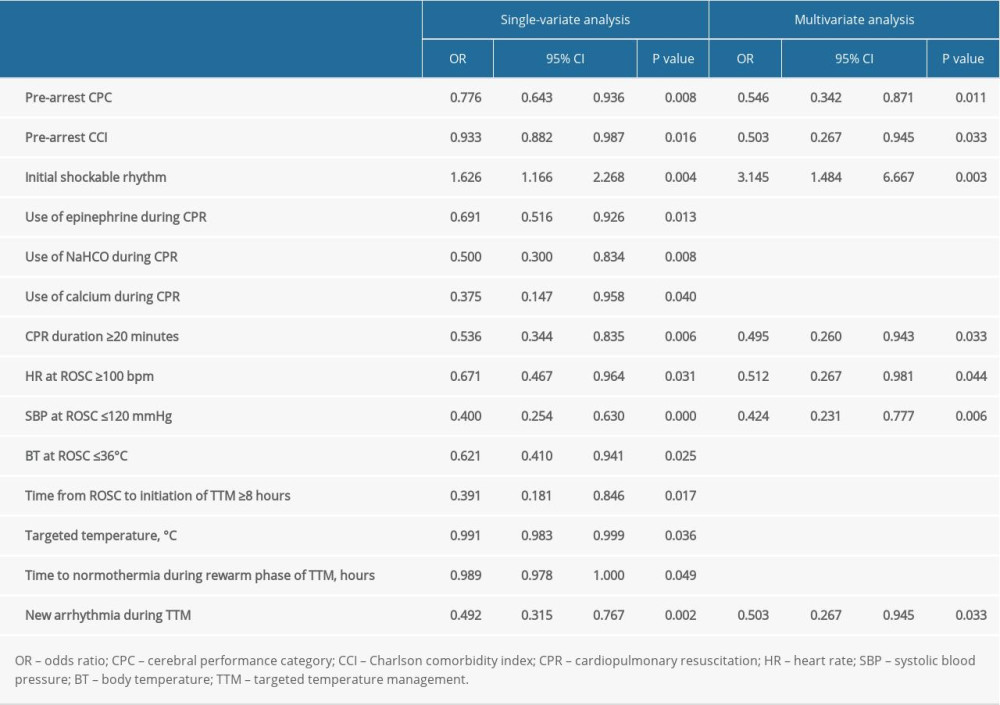 Table 4B. Predictors of good neurological outcome at hospital discharge among patients receiving targeted temperature control.
Table 4B. Predictors of good neurological outcome at hospital discharge among patients receiving targeted temperature control.
References
1. Chen C-T, Chiu P-C, Tang C-Y, Prognostic factors for survival outcome after in-hospital cardiac arrest: An observational study of the oriental population in Taiwan: J Chin Med Assoc, 2016; 79(1); 11-16
2. Radeschi G, Mina A, Berta G, Incidence and outcome of in-hospital cardiac arrest in Italy: A multicentre observational study in the Piedmont Region: Resuscitation, 2017; 119; 48-55
3. Girotra S, Nallamothu BK, Spertus JA, Trends in survival after in-hospital cardiac arrest: N Engl J Med, 2012; 367(20); 1912-20
4. Thompson LE, Chan PS, Tang F, Long-term survival trends of medicare patients after in-hospital cardiac arrest: Insights from get with the guidelines-resuscitation(®): Resuscitation, 2018; 123; 58-64
5. Moskowitz A, Holmberg MJ, Donnino MW, Berg KM, In-hospital cardiac arrest: Are we overlooking a key distinction?: Curr Opin Crit Care, 2018; 24(3); 151-57
6. Chen C-T, Chen C-H, Chen T-Y, Comparison of in-hospital and out-of-hospital cardiac arrest patients receiving targeted temperature management: A matched case-control study: J Chin Med Assoc, 2020; 83(9); 858-64
7. Lundbye JB, Rai M, Ramu B, Therapeutic hypothermia is associated with improved neurologic outcome and survival in cardiac arrest survivors of non-shockable rhythms: Resuscitation, 2012; 83(2); 202-7
8. Nadkarni VM, Larkin GL, Peberdy MA, First documented rhythm and clinical outcome from in-hospital cardiac arrest among children and adults: JAMA, 2006; 295(1); 50-57
9. Mandigers L, Termorshuizen F, de Keizer NF, A nationwide overview of 1-year mortality in cardiac arrest patients admitted to intensive care units in the Netherlands between 2010 and 2016: Resuscitation, 2020; 147; 88-94
10. Australia and New Zealand Cardiac Arrest Outcome and Determinants of ECMO (ANZ-CODE) Investigators, The epidemiology of in-hospital cardiac arrests in Australia: A prospective multicentre observational study: Crit Care Resusc, 2019; 21(3); 180-87
11. Saigal S, Sharma JP, Dhurwe R, Targeted temperature management: Current evidence and practices in critical care: Indian J Crit Care Med, 2015; 19(9); 537-46
12. Weng Y, Sun S, Therapeutic hypothermia after cardiac arrest in adults: Mechanism of neuroprotection, phases of hypothermia, and methods of cooling: Crit Care Clin, 2012; 28(2); 231-43
13. Polderman KH, Mechanisms of action, physiological effects, and complications of hypothermia: Crit Care Med, 2009; 37(7 Suppl); S186-202
14. Polderman KH, Herold I, Therapeutic hypothermia and controlled normothermia in the Intensive Care Unit: Practical considerations, side effects, and cooling methods: Crit Care Med, 2009; 37(3); 1101-20
15. Bernard SA, Gray TW, Buist MD, Treatment of comatose survivors of out-of-hospital cardiac arrest with induced hypothermia: N Engl J Med, 2002; 346(8); 557-63
16. Hypothermia after Cardiac Arrest Study Group, Mild therapeutic hypothermia to improve the neurologic outcome after cardiac arrest: N Engl J Med, 2002; 346(8); 549-56 [Erratum in: N Engl J. 2002;346(22): 1756]
17. Testori C, Sterz F, Behringer W, Mild therapeutic hypothermia is associated with favourable outcome in patients after cardiac arrest with non-shockable rhythms: Resuscitation, 2011; 82(9); 1162-67
18. Zhu Y, Huang H, Feng J, Ren Y, Li W, Therapeutic hypothermia for cardiac arrest due to non-shockable rhythm: A protocol for systematic review and meta-analysis: Medicine (Baltimore), 2020; 99(35); e21452
19. Nielsen N, Wetterslev J, Cronberg T, Targeted temperature management at 33°C versus 36°C after cardiac arrest: N Engl J Med, 2013; 369(23); 2197-206
20. Lascarrou J-B, Merdji H, Le Gouge A, Targeted temperature management for cardiac arrest with nonshockable rhythm: N Engl J Med, 2019; 381(24); 2327-37
21. Nolan Jerry P, Maconochie I, Soar J, Executive summary: 2020 International consensus on cardiopulmonary resuscitation and emergency cardiovascular care science with treatment recommendations: Circulation, 2020; 142(16 Suppl 1); S2-S27
22. Berg KM, Cheng A, Panchal AR, Part 7: Systems of care: 2020 American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care: Circulation, 2020; 142(16 Suppl 2); S580-S604
23. Mikkelsen ME, Christie JD, Abella BS, Use of therapeutic hypothermia after in-hospital cardiac arrest: Crit Care Med, 2013; 41(6); 1385-95
24. Wang CJ, Yang SH, Chen CH, Chung HP, Targeted temperature management for in-hospital cardiac arrest: 6 years of experience: Ther Hypothermia Temp Manag, 2020; 10(3); 153-58
25. Wang CH, Huang CH, Chang WT, Outcomes of adult in-hospital cardiac arrest treated with targeted temperature management: A retrospective cohort study: PLoS One, 2016; 11(11); e0166148
26. Nichol G, Huszti E, Kim F, Does induction of hypothermia improve outcomes after in-hospital cardiac arrest?: Resuscitation, 2013; 84(5); 620-25
27. Kory P, Fukunaga M, Mathew JP, Outcomes of mild therapeutic hypothermia after in-hospital cardiac arrest: Neurocrit Care, 2012; 16(3); 406-12
28. Chan PS, Berg RA, Tang Y, Curtis LH, Spertus JA, Association between therapeutic hypothermia and survival after in-hospital cardiac arrest: JAMA, 2016; 316(13); 1375-82
29. Polderman Kees H, Varon J, Confusion around therapeutic temperature management hypothermia after in-hospital cardiac arrest?: Circulation, 2018; 137(3); 219-21
30. Engsig M, Søholm H, Folke F, Similar long-term survival of consecutive in-hospital and out-of-hospital cardiac arrest patients treated with targeted temperature management: Clin Epidemiol, 2016; 8; 761-68
31. Chiu WT, Lin KC, Tsai MS, Post-cardiac arrest care and targeted temperature management: A consensus of scientific statement from the Taiwan Society of Emergency & Critical Care Medicine, Taiwan Society of Critical Care Medicine and Taiwan Society of Emergency Medicine: J Formos Med Assoc, 2021; 120(1 Pt 3); 569-87
32. D’Hoore W, Bouckaert A, Tilquin C, Practical considerations on the use of the Charlson comorbidity index with administrative data bases: J Clin Epidemiol, 1996; 49(12); 1429-33
33. Deyo RA, Cherkin DC, Ciol MA, Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases: J Clin Epidemiol, 1992; 45(6); 613-19
34. Yu Y, Meng Q, Munot S, Nguyen TN, Assessment of community interventions for bystander cardiopulmonary resuscitation in out-of-hospital cardiac arrest: A systematic review and meta-analysis: JAMA Network Open, 2020; 3(7); e209256
35. Rohlin O, Taeri T, Netzereab S, Duration of CPR and impact on 30-day survival after ROSC for in-hospital cardiac arrest-A Swedish cohort study: Resuscitation, 2018; 132; 1-5
36. Huang CH, Tsai MS, Ong HN, Association of hemodynamic variables with in-hospital mortality and favorable neurological outcomes in post-cardiac arrest care with targeted temperature management: Resuscitation, 2017; 120; 146-52
37. Perman SM, Stanton E, Soar J, Location of in-hospital cardiac arrest in the United States – variability in event rate and outcomes: J Am Heart Assoc, 2016; 5(10); e003638
Tables
Table 1. Baseline characteristics and pre-existing comorbidities of patients with IHCA and OHCA receiving targeted temperature.Table 2. Resuscitation-associated parameters and characteristics after return of spontaneous circulation of IHCA and OHCA patients receiving targeted temperature management.Table 3. Comparison of targeted temperature management related variables and clinical outcomes between patients with IHCA and OHCA.Table 4A. Predictors of survival to hospital discharge among patients receiving targeted temperature control in this cohort.Table 4B. Predictors of good neurological outcome at hospital discharge among patients receiving targeted temperature control. In Press
05 Mar 2024 : Clinical Research
Role of Critical Shoulder Angle in Degenerative Type Rotator Cuff Tears: A Turkish Cohort StudyMed Sci Monit In Press; DOI: 10.12659/MSM.943703
06 Mar 2024 : Clinical Research
Comparison of Outcomes between Single-Level and Double-Level Corpectomy in Thoracolumbar Reconstruction: A ...Med Sci Monit In Press; DOI: 10.12659/MSM.943797
21 Mar 2024 : Meta-Analysis
Economic Evaluation of COVID-19 Screening Tests and Surveillance Strategies in Low-Income, Middle-Income, a...Med Sci Monit In Press; DOI: 10.12659/MSM.943863
10 Apr 2024 : Clinical Research
Predicting Acute Cardiovascular Complications in COVID-19: Insights from a Specialized Cardiac Referral Dep...Med Sci Monit In Press; DOI: 10.12659/MSM.942612
Most Viewed Current Articles
17 Jan 2024 : Review article
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
14 Dec 2022 : Clinical Research
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387
01 Jan 2022 : Editorial
Editorial: Current Status of Oral Antiviral Drug Treatments for SARS-CoV-2 Infection in Non-Hospitalized Pa...DOI :10.12659/MSM.935952
Med Sci Monit 2022; 28:e935952