17 May 2021: Clinical Research
Association of Oral Behaviors with Anxiety, Depression, and Jaw Function in Patients with Temporomandibular Disorders in China: A Cross-Sectional Study
Lili Xu1ABCDE, Bin Cai1BCD, Shuai Fan1BCD, Shenji Lu1BCD, Kerong Dai2AD*DOI: 10.12659/MSM.929985
Med Sci Monit 2021; 27:e929985






Abstract
BACKGROUND: The aim of this study was to investigate the association of oral behaviors (OBs) with anxiety, depression, and jaw function in patients with temporomandibular disorders (TMDs) in China.
MATERIAL AND METHODS: A total of 537 patients diagnosed with TMD were included in this study (average age, 31.55±12.08 years; 86 men [16.0%] and 451 women [84.0%]). There were 31 cases of masticatory muscle pain, 459 cases of disc displacement, and 13 cases of arthralgia/arthrosis, and 34 cases were uncategorized. Patients were assessed using the Oral Behaviors Checklist (OBC), Jaw Functional Limitation Scale (JFLS), Generalized Anxiety Disorder-7 (GAD-7) scale, and Patient Health Questionnaire-9 (PHQ-9). The relationships between OBC scores and mouth opening, pain scores, JFLS, PHQ-9, and GAD-7 were evaluated with Spearman’s correlation analysis. The median TMD symptom duration was 3 (0.5-154) months; men and women did not differ significantly in symptom duration or in the number of episodes of depression and anxiety.
RESULTS: The following OBs were common in patients with TMDs: “putting pressure on the jaw (52.9%)”, “chewing food on 1 side (47.5%)”, and “holding teeth together during activities other than eating (33.3%)”. The OBC scores were significantly correlated with the JFLS, PHQ-9, and GAD-7 scores (P<0.01).
CONCLUSIONS: Patients with TMDs exhibit specific OBs, which are associated with depression, anxiety, and jaw function. It is necessary to further investigate the interaction of OBs with depression and anxiety in the development of TMDs.
Keywords: Anxiety, Depression, Jaw Abnormalities, Temporomandibular Joint Disorders, Adolescent, Behavior, Cross-Sectional Studies, Eating, Jaw, Mastication, young adult
Background
Temporomandibular disorders (TMDs) are a group of diseases with complex pathogenic factors, including malocclusion, craniofacial trauma, neurological and psychological factors, and oral behaviors (OBs) [1]. OBs, or oral parafunctions, mainly refer to activities other than normal oral physiological functions. They include activities such as chewing gum, clenching teeth, biting nails, and leaning the jaw on the hand, which may lead to TMDs. Studies in some disease models with OBs as causative factors of TMDs indicate that OBs can affect the masticatory musculature, resulting in tissue injury around the temporomandibular joint, pain, and functional limitations [2]. Additionally, OBs can cause stomatognathic microtrauma, particularly in the temporomandibular joint. Leketas et al found that OBs, such as clenching teeth, bruxism, tensing of the muscles, and sustained talking, are associated with TMDs [3].
However, it has been reported that OBs, or oral parafunctions, are not only risk factors for, but also are consequences of TMDs. Some bio-behavioral studies [4,5] have pointed out that psychosocial factors such as stress, depression, and anxiety play an important role in the occurrence and development of TMDs. Psychological stress in the form of anxiety and depression can increase OBs such as bruxism [6] and teeth clenching. A previous analysis [7] revealed that the incidence of oral parafunctions increased in individuals with depressive symptoms, possibly due to their fear-avoidance behavior. Therefore, OBs can be a sign of psychological stress and should not be regarded simply as a cause of disease.
Studies have focused mainly on specific OBs such as nail or lip biting, unilateral masticatory habit, and playing musical instruments that require certain mouth and chin positions, but the frequencies and characteristics of different OBs were not described in detail. This makes it difficult to compare the data between different studies. The Oral Behaviors Checklist (OBC) [8] comprises 21 items that evaluate the presence and frequency of OBs during night and day times, and semi-quantitative scoring was performed according to the frequency of OBs. The Diagnostic Criteria for Temporomandibular Disorders (DC/TMD) [9] recommends the use of OBC to screen patients for OBs and states that this checklist can be used for the complete study of OB characteristics in patients with TMDs.
To date, the OB characteristics of patients with TMDs have mostly been ignored, and only a few studies have assessed the relationships of OBs with depression, anxiety, and limited jaw function in Chinese patients. The Orofacial Pain Prospective Evaluation and Risk Assessment (OPPERA) study [1] showed that the characteristics of TMD-related symptoms have no significant differences between male and female patients with TMDs, but only a few studies have compared the differences of OBs between the sexes. This cross-sectional study aimed to examine the OB characteristics of patients with TMDs in China and further evaluate their correlation with jaw function, pain, mouth opening, depression, and anxiety.
Material and Methods
STUDY SETTING AND PARTICIPANTS:
This cross-sectional study included 537 consecutive patients with TMDs who visited the Ninth People’s Hospital between July 2017 and May 2018. The study was approved by the Ethics Committee of the Ninth People’s Hospital (No. 2016-114-T63; Clinical Trials Registration Number: ChiCTR-INR-16009881). The study procedures were in compliance with the Declaration of Helsinki. All participants provided informed consent to participate in the study.
Inclusion criteria were a diagnosis of TMD in accordance with DC/TMD [9], and completion of the assessments consisting of the OBC, Jaw Functional Limitation Scale (JFLS), Patient Health Questionnaire-9 (PHQ-9), and Generalized Anxiety Disorder-7 (GAD-7) scale. Exclusion criteria included a history of face or head trauma; facial or cranial fractures in the previous 10 years; rheumatoid arthritis, psoriatic arthritis, gout, or other systemic diseases that can affect the masticatory system; and oncologic or inflammatory diseases of the face or jaw.
MEASUREMENTS:
The Chinese version of the OBC, a self-reported questionnaire used to identify and quantify the frequency of different OBs, was obtained from
Jaw function was assessed using the JFLS [10], and the GAD-7 [11] and PHQ-9 [12] were used to evaluate anxious and depressive moods, respectively, in patients with TMDs [9]. The total GAD-7 score ranges from 0 to 21, and the total PHQ-9 score ranges from 0 to 27. Anxiety and depression in patients were defined as a GAD-7 score ≥10 and a PHD-9 score ≥10, respectively. Patients completed these questionnaires during the first treatment session. All patient queries regarding the questionnaires were resolved by the assessor to ensure that patients completely understood the questions.
The examinations of all enrolled patients were completed by investigators who had more than 5 years of experience in diagnosing patients with TMDs. The investigators asked specific questions pertaining to the patients’ pain and examined mouth opening and closing, range of motion of the jaw, and the position of pain. The maximum painless mouth opening (in mm) was measured, and the pain was assessed by a numeric rating scale ranging from 0 to 10.
STATISTICAL ANALYSIS:
Statistical analyses were performed using SPSS, version 23 (IBM Corp., Armonk, NY, USA). The frequencies of specific OBs were analyzed based on the total number of subjects with those OBs. Descriptive statistics were presented as mean±standard deviation. To measure internal consistency, Cronbach’s alpha (α) of the Chinese version of the OBC was used, with α >0.7 indicating good reliability. The rank-sum test was used to show the sex distribution of individual OBs in patients with TMDs. The correlations between GAD-7, PHQ-9, jaw function, pain score, mouth opening, and OBC score were analyzed by Spearman’s correlation. Because 5 comparisons were made, statistical significance for 2-sided statistical testing was set at α=0.05/5=0.01.
Results
This study included 537 patients with TMDs (average age, 31.55±12.08 years; range, 15–68 years; 86 men [16.0%] and 451 women [84.0%]). The median TMD symptom duration was 3 (0.5–154) months; the symptom duration and the number of episodes of anxiety and depression did not differ significantly between men and women. Details of the patients’ diagnostic classification are shown in Table 1. The internal consistency of OBC scores was α=0.771 for the entire study sample. The total OBC score was calculated and categorized as follows [13]: 0 to 16 (29.0%), 17 to 24 (27.7%), and ≥25 (43.2%) (Table 1).
To determine the most common OBs, the scores were dichotomized. If the patient chose “most of the time” or “all of the time” for a specific item, it was considered that the patient had that OB (Table 2). More than half of the patients with TMDs reported that they were sleeping in a position that could exert pressure on the jaw (52.9%). Moreover, “chewing food unilaterally”, “clenching, touching, or holding the teeth together during activities other than eating”, “yawning”, and “eating between meals” were very common behaviors in patients with TMD. The total OBC scores differed significantly between men and women (
Depression and anxiety symptoms were observed in 14.5% and 10.2% of patients with TMDs, respectively (Table 1). Generally, the total OBC score correlated significantly with the JFLS, PHQ-9, and GAD-7 scores (
Discussion
This study showed that patients with TMDs do have certain OBs, such as “pressing, touching, or holding the teeth together during activities other than eating”, “chewing food on 1 side”, and “putting pressure on the jaw”. These results were basically consistent with those of Leketas et al [3]. Certain OBs such as “grinding teeth while awake”, “tightening or tensing muscles”, and “talking for a long time” could increase the risk of TMDs [14]. However, most previous studies have examined only a small number of OBs, such as chewing gum, bruxism, and thumb-sucking [15,16]. The use of the OBC in this study allowed the evaluation of a wider spectrum of OBs.
The OBC uses scores of 0 to 4, graded according to the frequency of the OBs, which allows semi-quantitative analysis. A score of 3 or 4 indicated that the patient had that particular oral habit. This semi-quantitative scoring helps the patients choose the appropriate answer, and thus reflects OB characteristics more accurately. Recently, different language versions of the OBC [17,18] have been used clinically, with good reliability for OB evaluation. The Chinese version of the OBC used in this study also had good reliability (Cronbach’s α=0.771).
Different OBs can increase the load of the temporomandibular joint and cause some pathological changes in the joint and its surrounding tissues. Pressure in the temporomandibular joint cavity is the highest in the maximal intercuspal position [19], and the pressure on the side of the articular disc increases [20] when the teeth are clenched [21], which can lead to articular disc injury. Masumeh et al [22] reported that eating hard food is more likely to induce unilateral chewing than is eating soft food, as the bite force may differ between sides. When chewing hard food, patients tend to use the dominant side. A cone-beam computed tomography-based study [23] found that individuals with unilateral chewing function, compared with individuals without this function, had the following manifestations on the chewing side: (1) narrower posterosuperior, posterior, and lateral joint spaces; (2) shorter condylar neck; and (3) smaller inclination of the articular eminence. The increase of excessive stress in articular cartilage can lead to the increase of degradation of type II collagen and proliferation of type III collagen [24], which may be related to the pathogenesis of TMD. In this study, “chewing food on 1 side” (47.5%),” “pressing, touching, or holding the teeth together during activities other than eating (33.3%),” and “clenching or grinding teeth when asleep (22.5%)” habits theoretically increased the daily load and mechanical stress on the temporomandibular joint, which may be related to degeneration of the joint.
The male-to-female ratio in this study was approximately 1: 5, and, compared with men, women with TMDs showed less mouth opening, more severe pain, and more limited jaw functions (
Studies have indicated that depression and anxiety may be risk factors for TMD-related pain [25]. Psychological factors such as psychological distress, pain catastrophizing [26], fear-avoidance behaviors [27], depression and anxiety [28], and passive coping strategies [29] are associated with the increased pain and disability levels in patients with painful TMDs. Depression and anxiety have been documented to influence muscular activities [30]. This can disturb the harmonization among the closely matched muscles around the joint and induce changes in their mechanical properties, eventually resulting in muscle pain. This condition can also initiate inflammatory reactions in the joint, eliciting secondary biomechanical changes and joint pain. Simultaneously, patients with TMDs can have abnormal trigeminal pain processes [31], which may be related to an imbalance of 5-hydroxytryptamine and catecholamine neurotransmitters. Therefore, psychological or emotional problems are also involved in the pathogenesis of TMDs, emphasizing the significance of mental state evaluation.
In this study, the total OBC score correlated with depression and anxiety (r=0.375 and 0.322, respectively;
Conclusions
The results of this pilot study suggest that there are differences in OBs between men and women with TMDs, which may be related to the severity of symptoms. OBs were associated with depression, anxiety, and limited jaw function. These factors may have complex interactions and change with the development of the disease. Thus, additional cohort studies are warranted to further explore these relationships.
Tables
Table 1. Duration of symptoms, depression, anxiety, oral behaviors, jaw function, mouth opening, pain, and social status in male and female patients with temporomandibular disorders. Table 2. Prevalence of oral behaviors in male and female patients with temporomandibular disorders.
Table 2. Prevalence of oral behaviors in male and female patients with temporomandibular disorders.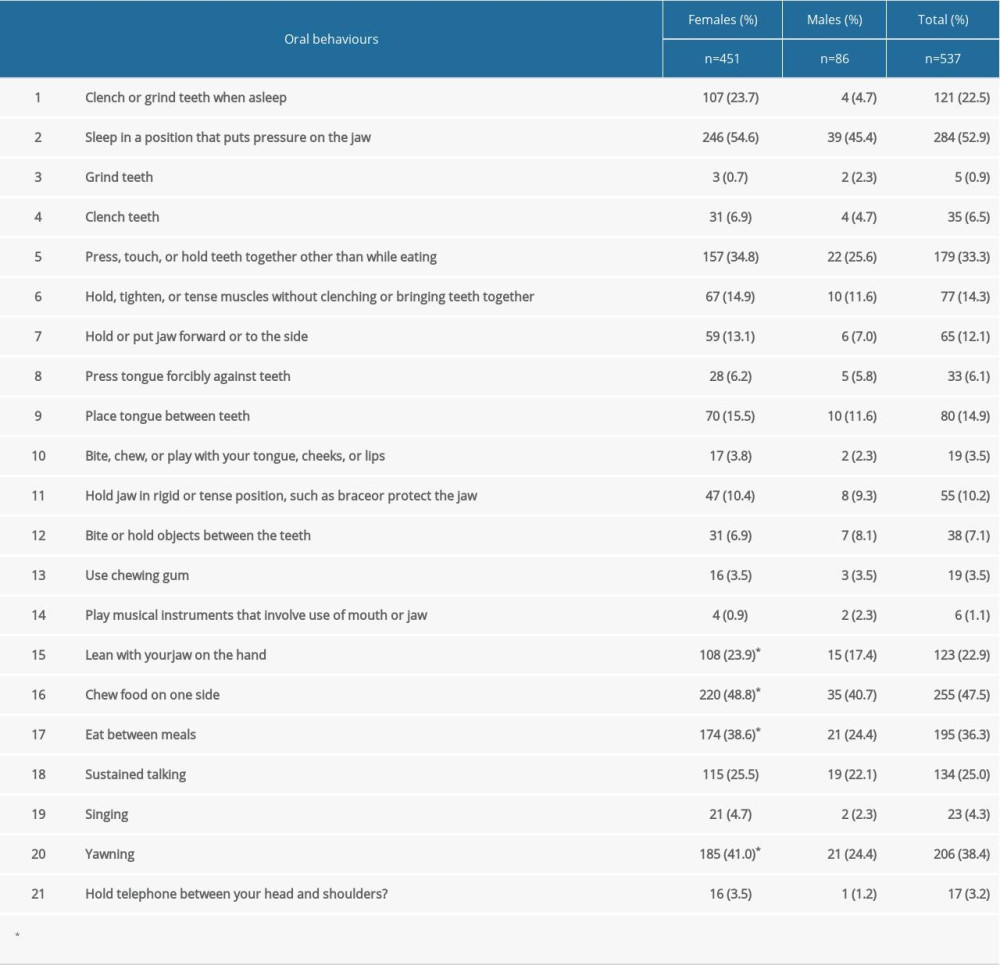 Table 3. Spearman correlations among OBC, JFLS, GAD-7 scale, and PHQ-9.
Table 3. Spearman correlations among OBC, JFLS, GAD-7 scale, and PHQ-9.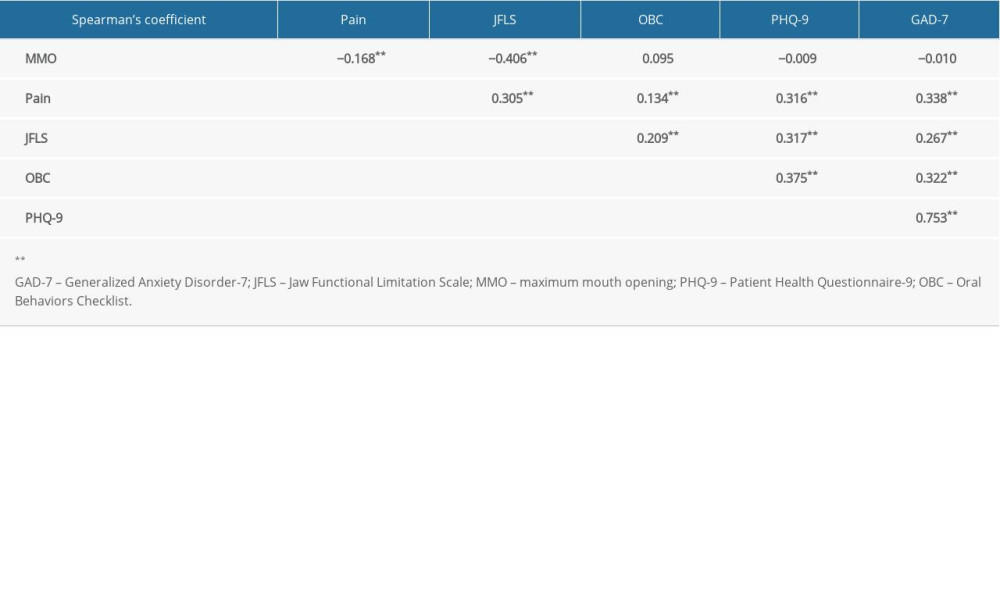
References
1. Slade GD, Ohrbach R, Greenspan JD, Painful temporomandibular disorder: Decade of discovery from OPPERA studies: J Dent Res, 2016; 95(10); 1084-92
2. Glaros AG, Hanson AH, Ryen CC, Headache and oral parafunctional behaviors: Appl Psychophysiol Biofeedback, 2014; 39(1); 59-66
3. Leketas M, Saferis V, Kubilius R, Oral behaviors and parafunctions: Comparison of temporomandibular dysfunction patients and controls: J Craniofac Surg, 2017; 28(8); 1933-38
4. Canales GT, Guarda-Nardini L, Rizzatti-Barbosa CM, Distribution of depression, somatization and pain-related impairment in patients with chronic temporomandibular disorders: J Appl Oral Sci, 2019; 27; e20180210
5. Jeremic-Knezevic M, Knezevic A, Boban N, Correlation of somatization, depression, and chronic pain with clinical findings of the temporomandibular disorders in asymptomatic women: Cranio, 2021; 39(1); 17-23
6. van Selms MK, Muzalev K, Visscher CM, Are pain-related temporomandibular disorders the product of an interaction between psychological factors and self-reported bruxism?: J Oral Facial Pain Headache, 2017; 31(4); 331-38
7. Khawaja SN, Nickel JC, Iwasaki LR, Association between waking-state oral parafunctional behaviors and bio-psychosocial characteristics: J Oral Rehabil, 2015; 42(9); 651-56
8. Markiewicz MR, Ohrbach R, McCall WD, Oral behaviors checklist: Reliability of performance in targeted waking-state behaviors: J Orofac Pain, 2006; 20(4); 306-16
9. Schiffman E, Ohrbach R, Truelove E, Diagnostic Criteria for Temporomandibular Disorders (DC/TMD) for Clinical and Research Applications: Recommendations of the International RDC/TMD Consortium Network* and Orofacial Pain Special Interest Groupdagger: J Oral Facial Pain Headache, 2014; 28(1); 6-27
10. Xu L, He Y, Fan S, Validation of a Chinese version of the Jaw Functional Limitation Scale in relation to the diagnostic subgroup of temporomandibular disorders: J Oral Rehabil, 2020; 47(1); 1-8
11. Spitzer RL, Kroenke K, Williams JB, Lowe B, A brief measure for assessing generalized anxiety disorder: The GAD-7: Arch Intern Med, 2006; 166(10); 1092-97
12. Kroenke K, Spitzer RL, Williams JB, The PHQ-9: Validity of a brief depression severity measure: J Gen Intern Med, 2001; 16(9); 606-13
13. Ohrbach R, Fillingim RB, Mulkey F, Clinical findings and pain symptoms as potential risk factors for chronic TMD: Descriptive data and empirically identified domains from the OPPERA case-control study: J Pain, 2011; 12(11 Suppl); T27-45
14. Michelotti A, Cioffi I, Festa P, Oral parafunctions as risk factors for diagnostic TMD subgroups: J Oral Rehabil, 2010; 37(3); 157-62
15. Jimenez-Silva A, Pena-Duran C, Tobar-Reyes J, Frugone-Zambra R, Sleep and awake bruxism in adults and its relationship with temporomandibular disorders: A systematic review from 2003 to 2014: Acta Odontol Scand, 2017; 75(1); 36-58
16. Mejersjo C, Ovesson D, Mossberg B, Oral parafunctions, piercing and signs and symptoms of temporomandibular disorders in high school students: Acta Odontol Scand, 2016; 74(4); 279-84
17. Barbosa C, Manso MC, Reis T, Cultural equivalence, reliability and utility of the Portuguese version of the Oral Behaviors Checklist: J Oral Rehabil, 2018; 45(12); 924-31
18. Donnarumma V, Cioffi I, Michelotti A, Analysis of the reliability of the Italian version of the Oral Behaviors Checklist and the relationship between oral behaviors and trait anxiety in healthy individuals: J Oral Rehabil, 2018; 45(4); 317-22
19. Casares G, Thomas A, Carmona J, Influence of oral stabilization appliances in intra-articular pressure of the temporomandibular joint: Cranio, 2014; 32(3); 219-23
20. Aoun M, Mesnard M, Monede-Hocquard L, Ramos A, Stress analysis of temporomandibular joint disc during maintained clenching using a viscohyperelastic finite element model: J Oral Maxillofac Surg, 2014; 72(6); 1070-77
21. Commisso MS, Martinez-Reina J, Mayo J, A study of the temporomandibular joint during bruxism: Int J Oral Sci, 2014; 6(2); 116-23
22. Zamanlu M, Khamnei S, Salarilak S, Chewing side preference in first and all mastication cycles for hard and soft morsels: Int J Clin Exp Med, 2012; 5(4); 326-31
23. Jiang H, Li C, Wang Z, Assessment of osseous morphology of temporomandibular joint in asymptomatic participants with chewing-side preference: J Oral Rehabil, 2015; 42(2); 105-12
24. Zhang C, Xu Y, Cheng Y, Effect of asymmetric force on the condylar cartilage, subchondral bone and collagens in the temporomandibular joints: Arch Oral Biol, 2015; 60(4); 650-63
25. Kindler S, Samietz S, Houshmand M, Depressive and anxiety symptoms as risk factors for temporomandibular joint pain: A prospective cohort study in the general population: J Pain, 2012; 13(12); 1188-97
26. Velly AM, Look JO, Carlson C, The effect of catastrophizing and depression on chronic pain – a prospective cohort study of temporomandibular muscle and joint pain disorders: Pain, 2011; 152(10); 2377-83
27. Gil-Martinez A, Grande-Alonso M, Lopez-de-Uralde-Villanueva I, Chronic temporomandibular disorders: disability, pain intensity and fear of movement: J Headache Pain, 2016; 17(1); 103
28. Diracoglu D, Yildirim NK, Saral I, Temporomandibular dysfunction and risk factors for anxiety and depression: J Back Musculoskelet Rehabil, 2016; 29(3); 487-91
29. Fillingim RB, Ohrbach R, Greenspan JD, Psychological factors associated with development of TMD: The OPPERA prospective cohort study: J Pain, 2013; 14(12 Suppl); T75-90
30. Stocka A, Sierpinska T, Kuc J, Golebiewska M, Relationship between depression and masticatory muscles function in a group of adolescents: Cranio, 2018; 36(6); 390-95
31. Brazoloto TM, de Siqueira SR, Rocha-Filho PA, Post-operative orofacial pain, temporomandibular dysfunction and trigeminal sensitivity after recent pterional craniotomy: Preliminary study: Acta Neurochirurgica, 2017; 159(5); 799-805
Tables
Table 1. Duration of symptoms, depression, anxiety, oral behaviors, jaw function, mouth opening, pain, and social status in male and female patients with temporomandibular disorders.Table 2. Prevalence of oral behaviors in male and female patients with temporomandibular disorders.Table 3. Spearman correlations among OBC, JFLS, GAD-7 scale, and PHQ-9. In Press
05 Mar 2024 : Clinical Research
Role of Critical Shoulder Angle in Degenerative Type Rotator Cuff Tears: A Turkish Cohort StudyMed Sci Monit In Press; DOI: 10.12659/MSM.943703
06 Mar 2024 : Clinical Research
Comparison of Outcomes between Single-Level and Double-Level Corpectomy in Thoracolumbar Reconstruction: A ...Med Sci Monit In Press; DOI: 10.12659/MSM.943797
21 Mar 2024 : Meta-Analysis
Economic Evaluation of COVID-19 Screening Tests and Surveillance Strategies in Low-Income, Middle-Income, a...Med Sci Monit In Press; DOI: 10.12659/MSM.943863
10 Apr 2024 : Clinical Research
Predicting Acute Cardiovascular Complications in COVID-19: Insights from a Specialized Cardiac Referral Dep...Med Sci Monit In Press; DOI: 10.12659/MSM.942612
Most Viewed Current Articles
17 Jan 2024 : Review article
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
14 Dec 2022 : Clinical Research
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387
01 Jan 2022 : Editorial
Editorial: Current Status of Oral Antiviral Drug Treatments for SARS-CoV-2 Infection in Non-Hospitalized Pa...DOI :10.12659/MSM.935952
Med Sci Monit 2022; 28:e935952